
 Events
Events Latest images
Latest imagesDa remiziram...vol II.
Page 13 of 50
Page 13 of 50 •  1 ... 8 ... 12, 13, 14 ... 31 ... 50
1 ... 8 ... 12, 13, 14 ... 31 ... 50 ![]()

Eroo- Posts : 78946
2016-07-22

Re: Da remiziram...vol II.
 by Hektorović 13/3/2021, 18:08
by Hektorović 13/3/2021, 18:08
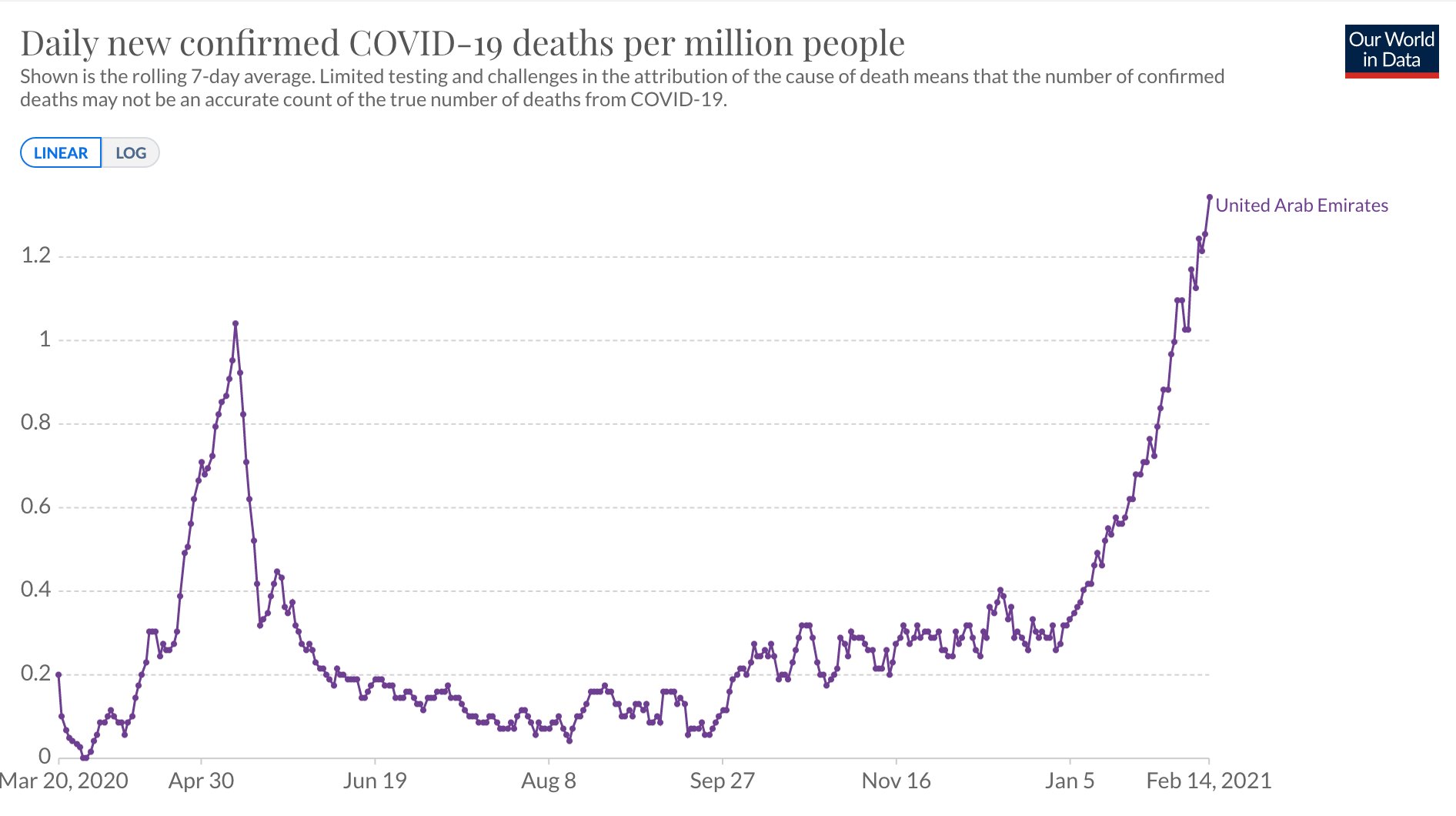
Dakle nakon punih godinu od prvog slučaja, i nakon što de facto nisu imali lockdown i skoro nikakve mjere još od 5 mjeseca prošle godine...
Maske obavezne na otvorenom u Banjaluci, zabranjena okupljanja
Foto: Ilustracija | Maske obavezne na otvorenom u Banjaluci, zabranjena okupljanja
"Sve epidemiološke mjere koje su trenutno na snazi ostaju i dalje, do 18. marta", navedeno je u saopštenju nakon sjednice.
Kako se dodaje u zaključcima, koji su doneseni jednoglasno, građani su obavezni da se pridržavaju zaštitne mjere fizičkog rastojanja od dva metra, osim u slučaju da se osoba kreće sama, sa članovima porodice ili tokom obavljanja fizičke aktivnosti.
Kako se navodi u saopštenju trenutna epidemiološka situacija u Banjaluci je nepovoljna, sa tendencijom daljeg pogoršavanja. Zabilježen je povećan broj građana koji su pozitivni na virus korona.
Kako se dodaje zaključak je i da se uputi jasna instrukcija i opomena svim obrazovnim i kulturnim ustanovama da se obavezno poštuju epidemiološke mjere, uz napomenu da će se vršiti pojačana kontrola u narednom periodu.
"Obavezuju se svi tržni centri i marketi da na vidnom mjestu istaknu broj ljudi koji može biti unutra, a to je jedno lice na četiri kvadrata, te da kontrolišu ulazak i izlazak uz obaveznu dezinfekciju. Zabranjuju se bilo kakva okupljanja unutar istih. Gradski kontrolni organi moraju pojačati kontrolu provođenja ove mjere. Ova mjera odnosi se i na sve pijace", pojašnjeno je u saopštnju.
Kako se navodi Gradski štab će uputiti prijedlog Republičkom štabu da se za ulazak u Republiku Srpsku/Bosnu i Hercegovinu uvede obavezan PCR test, osim za građane Republike Srbije.
"Obavezuju se direktori osnovnih i srednjih škola, kao i vrtića da dostavljaju izvještaje o epidemiološkoj situaciji na dnevnom nivou. U saradnji sa Ministarstvom prosvjete i kulture RS razmotriti mjeru obustavljanja nastave u osnovnim školama (od 5 do 9 razreda), ukoliko se loša epidemiološka situacija nastavi", takođe je jedan od zaključaka.
Naređena je i dezinfekcija javnih površina, javnih saobraćajnica u centralnom gradskom području i parkinzi, dječijih igrališta i posebno prilaza školama.
"Pojačati kontrolu poštovanja propisanih mjera u gradskom saobraćaju", navedno je u saopštenju.
Gradska uprava je pozvala sugrađane na dodatni oprez i da se strogo pridržavaju propisanih epidemioloških mjera, jer svaka mjera ima efekta onoliko koliko se poštuje.
Štab za vanredne situacije grada Banjaluke nastaviće pratiti situaciju i u skladu s tim pravovremeno reagovati. Zbog pogoršane epidemiološke situacije, jedan dio članova danas je bio uključen onlajn, dok je jedan dio lično prisustvovao sjednici.
Sljedeća sjednica Štaba biće održana u srijedu ili četvrtak, a po potrebi i prije.
Maske obavezne na otvorenom u Banjaluci, zabranjena okupljanja
BANJALUKA - Štab za vanredne situacije grada Banjaluka na današnjoj sjednici donio je zaključak koji obavezuje građane da na otvorenom, kao i u zatvorenom prostoru obavezno nose zaštitnu masku, a do 18. marta su zabranjena sva javna i privatna okupljanja, saopštila je Gradska uprava.
Maja Brkić 13.03.2021 16:12Foto: Ilustracija | Maske obavezne na otvorenom u Banjaluci, zabranjena okupljanja
"Sve epidemiološke mjere koje su trenutno na snazi ostaju i dalje, do 18. marta", navedeno je u saopštenju nakon sjednice.
Kako se dodaje u zaključcima, koji su doneseni jednoglasno, građani su obavezni da se pridržavaju zaštitne mjere fizičkog rastojanja od dva metra, osim u slučaju da se osoba kreće sama, sa članovima porodice ili tokom obavljanja fizičke aktivnosti.
Kako se navodi u saopštenju trenutna epidemiološka situacija u Banjaluci je nepovoljna, sa tendencijom daljeg pogoršavanja. Zabilježen je povećan broj građana koji su pozitivni na virus korona.
Kako se dodaje zaključak je i da se uputi jasna instrukcija i opomena svim obrazovnim i kulturnim ustanovama da se obavezno poštuju epidemiološke mjere, uz napomenu da će se vršiti pojačana kontrola u narednom periodu.
"Obavezuju se svi tržni centri i marketi da na vidnom mjestu istaknu broj ljudi koji može biti unutra, a to je jedno lice na četiri kvadrata, te da kontrolišu ulazak i izlazak uz obaveznu dezinfekciju. Zabranjuju se bilo kakva okupljanja unutar istih. Gradski kontrolni organi moraju pojačati kontrolu provođenja ove mjere. Ova mjera odnosi se i na sve pijace", pojašnjeno je u saopštnju.
Kako se navodi Gradski štab će uputiti prijedlog Republičkom štabu da se za ulazak u Republiku Srpsku/Bosnu i Hercegovinu uvede obavezan PCR test, osim za građane Republike Srbije.
"Obavezuju se direktori osnovnih i srednjih škola, kao i vrtića da dostavljaju izvještaje o epidemiološkoj situaciji na dnevnom nivou. U saradnji sa Ministarstvom prosvjete i kulture RS razmotriti mjeru obustavljanja nastave u osnovnim školama (od 5 do 9 razreda), ukoliko se loša epidemiološka situacija nastavi", takođe je jedan od zaključaka.
Naređena je i dezinfekcija javnih površina, javnih saobraćajnica u centralnom gradskom području i parkinzi, dječijih igrališta i posebno prilaza školama.
"Pojačati kontrolu poštovanja propisanih mjera u gradskom saobraćaju", navedno je u saopštenju.
Gradska uprava je pozvala sugrađane na dodatni oprez i da se strogo pridržavaju propisanih epidemioloških mjera, jer svaka mjera ima efekta onoliko koliko se poštuje.
Štab za vanredne situacije grada Banjaluke nastaviće pratiti situaciju i u skladu s tim pravovremeno reagovati. Zbog pogoršane epidemiološke situacije, jedan dio članova danas je bio uključen onlajn, dok je jedan dio lično prisustvovao sjednici.
Sljedeća sjednica Štaba biće održana u srijedu ili četvrtak, a po potrebi i prije.

Hektorović- Posts : 26373
2018-04-10
Eroo- Posts : 78946
2016-07-22
Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Guest 14/3/2021, 15:51
evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809

Guest- Guest
Re: Da remiziram...vol II.
by mutava baštarda 14/3/2021, 16:02
nadao sam se da će na zapadu biti neka država koja je oaza od ove malo jače prehlade ili mutanta iz laboratorija, nebitno, a ono ispalo da milijarda Indijaca, a mogli bi reći i milijarda kineza i skoro cijela Afrika nemaju problema s koronom. Drug Tito kao jedan od osnivača Nesvrstanih bi ovaj virus nazvao bolešću kapitalizma...Gnječ wrote:evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
_________________
Iduća dva tjedna su ključna
mutava baštarda- Posts : 21037
2015-09-14
Re: Da remiziram...vol II.
by Guest 14/3/2021, 16:17
mutava baštarda wrote:nadao sam se da će na zapadu biti neka država koja je oaza od ove malo jače prehlade ili mutanta iz laboratorija, nebitno, a ono ispalo da milijarda Indijaca, a mogli bi reći i milijarda kineza i skoro cijela Afrika nemaju problema s koronom. Drug Tito kao jedan od osnivača Nesvrstanih bi ovaj virus nazvao bolešću kapitalizma...Gnječ wrote:evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
za vas koji čitate samo vijesti iz rvacke i bosanske mahale i raznih evropskih kasaba sigurno da indijci i kinezi nemaju problema sa virusom jer u mahala i eu kasaba medijima to ne piše a što u mahala i eu kasaba medijima ne piše znači da ne postoji. amen.
Guest- Guest
Re: Da remiziram...vol II.
by mutava baštarda 14/3/2021, 16:29
Ispravno se kaže u postkovid društvu Awomen.Gnječ wrote:mutava baštarda wrote:nadao sam se da će na zapadu biti neka država koja je oaza od ove malo jače prehlade ili mutanta iz laboratorija, nebitno, a ono ispalo da milijarda Indijaca, a mogli bi reći i milijarda kineza i skoro cijela Afrika nemaju problema s koronom. Drug Tito kao jedan od osnivača Nesvrstanih bi ovaj virus nazvao bolešću kapitalizma...Gnječ wrote:evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
za vas koji čitate samo vijesti iz rvacke i bosanske mahale i raznih evropskih kasaba sigurno da indijci i kinezi nemaju problema sa virusom jer u mahala i eu kasaba medijima to ne piše a što u mahala i eu kasaba medijima ne piše znači da ne postoji. amen.
_________________
Iduća dva tjedna su ključna
mutava baštarda- Posts : 21037
2015-09-14
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 19:54
Gnječ wrote:evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
Gnječo, ako se sjećaš u par navrata sam spominjao Istru kao dobar primjer za kontrolu širenja epidemije,
a ujedno sam upozorio na mogući "zamor", jer su i istrani krvavi ispod kože. Postotak kolektivne imunizacije
je u Istri izrazito nizak, niži od bilo koje regije u Europi, ali je zato i bazen za širenje virusa s time veći.
Čak sam i predlagao da se u slučaju Istre odstupi od načela "ravnomjernog cijepljenja, u skladu sa brojem
stanovnika po županijama". Sličan primjer smo imali i u Sloveniji - Primorska.Zbog blizine Italije tamo su se
ljudi od samog početka ponašali izrazito disciplinirano. No, na kraju se popustilo i ušlo se u fazu većeg
relativno većeg širenja virusa. Tipičan primjer gdje Donnelly- Fergusonov model u jednom dijelui odkaže, a na kraju se
može u nekom smislu potvrditi. Ipak se ovdje radi o ljudima i ne kravama po farmama. Faktor koji je zbog mnogo
toga veoma teško matematički modelirati.
Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 20:08
PS:
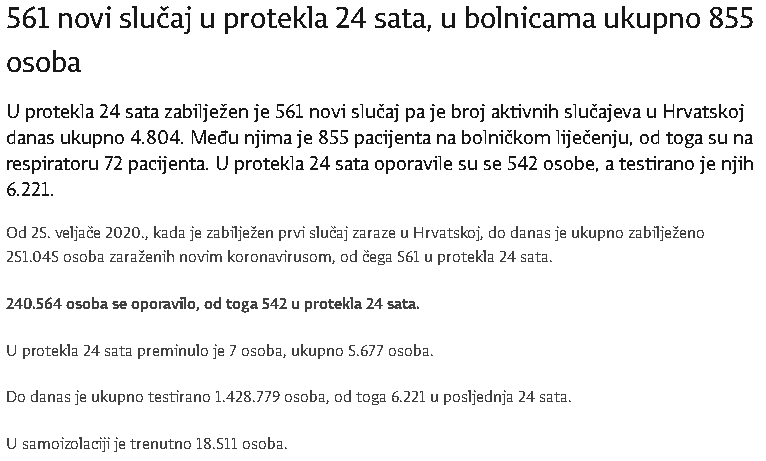
Danas je u HR u samoizolaciji 18,501 osoba. Ti ljudi su ili zdravi, ili sa blagim simptomima.
Kuda s njima? Kud bi ih ti dao. Moja snaha je čak i na PCR bila
pozitivna, s blagim simptomima -par dana malo temperature, malo kašlja,
gubitak vonja i to je to. Cijelo vrijeme je radila (veoma odgovoran posao ) online.
120 ljudi ni u jednom trenutku nisu bili bez njene podrške. Izolirala se u posebnoj sobi
i nije se petljala u život ostatka obitelji. Jelo je dobivala ispred vrata, da ne spominjem
ostale detalje.
Danas je u HR u samoizolaciji 18,501 osoba. Ti ljudi su ili zdravi, ili sa blagim simptomima.
Kuda s njima? Kud bi ih ti dao. Moja snaha je čak i na PCR bila
pozitivna, s blagim simptomima -par dana malo temperature, malo kašlja,
gubitak vonja i to je to. Cijelo vrijeme je radila (veoma odgovoran posao ) online.
120 ljudi ni u jednom trenutku nisu bili bez njene podrške. Izolirala se u posebnoj sobi
i nije se petljala u život ostatka obitelji. Jelo je dobivala ispred vrata, da ne spominjem
ostale detalje.
Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 20:14
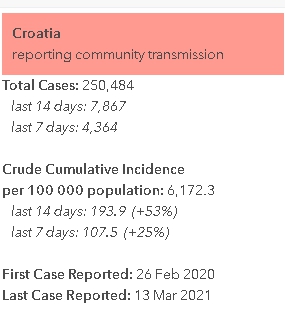
HR danas: 14.3.2021
7 dnevma kumulativa: 4531 ili prosječno +647/dan
7 dnevma kumulativa: 4531 ili prosječno +647/dan
_________________
Nulla rosa sine spina
Eroo- Posts : 78946
2016-07-22

max123- Posts : 2853
2015-10-28
Lokacija: : Zemun,Hrvatska
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 21:10
Dokaz da se do imuniteta krda ne može doći na prirodan način.
Sjeverne regije imaju dnevnu zarazu puno veću od prosjeka Italije,
odnosno južnih regija. Talijanima su razlozi zasigurno poznati.
Nije mi baš do kraja jasno zašto svoje spoznaje ne podijeli
s ostatkom svijeta. Baš šteta...

Sjeverne regije imaju dnevnu zarazu puno veću od prosjeka Italije,
odnosno južnih regija. Talijanima su razlozi zasigurno poznati.
Nije mi baš do kraja jasno zašto svoje spoznaje ne podijeli
s ostatkom svijeta. Baš šteta...
Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 21:45
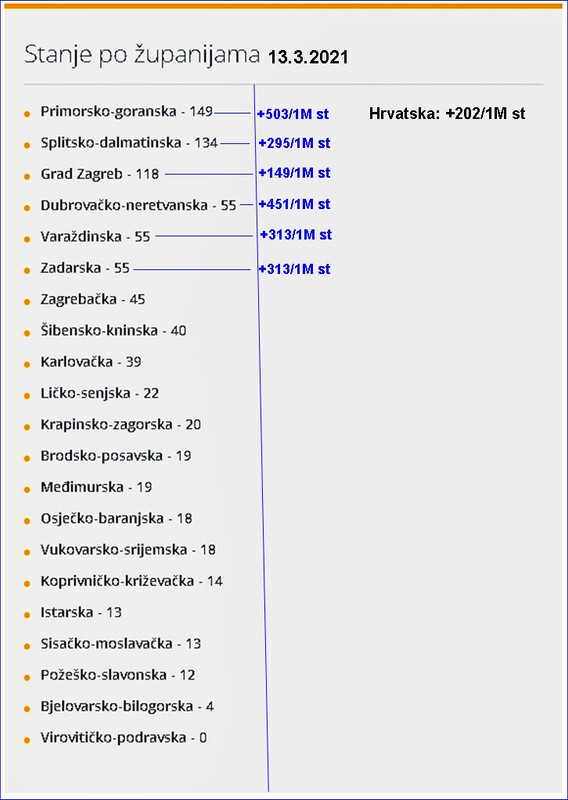
Današnji novozaraženi u Italiji i nekim dijelovima na sjeveru Italije: potvrđeni slučajevi na 1 milijun stanovnika!
Italija: +353/1M
Lombardia: +429/1M
Bergamo: 248/1M
Brescia: 834/1M
Udine: +629/1M
Udine su primjer kao oni koje sam negdje gore spomenuo: slovenska i hrvatska Istra, respektivno!
I dalje mi nije ništa jasno što se događa sa Brescijom (graniči na Bergamo!).
Za uspordbu Hrvatska: +138/1M. ....slika nije loša, ali se mora biti oprezan.
Slovenija: +250/1M ...evidentno je opadanje.
PS: Srbija +607/1M ....za BiH nije moguće ništa reći, zbog nesigurnih rezultata.
Italija: +353/1M
Lombardia: +429/1M
Bergamo: 248/1M
Brescia: 834/1M
Udine: +629/1M
Udine su primjer kao oni koje sam negdje gore spomenuo: slovenska i hrvatska Istra, respektivno!
I dalje mi nije ništa jasno što se događa sa Brescijom (graniči na Bergamo!).
Za uspordbu Hrvatska: +138/1M. ....slika nije loša, ali se mora biti oprezan.
Slovenija: +250/1M ...evidentno je opadanje.
PS: Srbija +607/1M ....za BiH nije moguće ništa reći, zbog nesigurnih rezultata.
Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Guest 14/3/2021, 23:01
Eroo wrote:Gnječ wrote:evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
Gnječo, ako se sjećaš u par navrata sam spominjao Istru kao dobar primjer za kontrolu širenja epidemije,
a ujedno sam upozorio na mogući "zamor", jer su i istrani krvavi ispod kože. Postotak kolektivne imunizacije
je u Istri izrazito nizak, niži od bilo koje regije u Europi, ali je zato i bazen za širenje virusa s time veći.
Čak sam i predlagao da se u slučaju Istre odstupi od načela "ravnomjernog cijepljenja, u skladu sa brojem
stanovnika po županijama". Sličan primjer smo imali i u Sloveniji - Primorska.Zbog blizine Italije tamo su se
ljudi od samog početka ponašali izrazito disciplinirano. No, na kraju se popustilo i ušlo se u fazu većeg
relativno većeg širenja virusa. Tipičan primjer gdje Donnelly- Fergusonov model u jednom dijelui odkaže, a na kraju se
može u nekom smislu potvrditi. Ipak se ovdje radi o ljudima i ne kravama po farmama. Faktor koji je zbog mnogo
toga veoma teško matematički modelirati.
a bokte, jel tebi ovako kao laiku ne izgleda apsurdno i totalno van svih medicinskih protokola poslati zaražene u samoizolaciju među nezaražene ljude? i onda se debili čude da imaju porast zaraženih? kakvog smisla imaju sve te njihove kurčeve mjere i zabrane kad stožer sam generira zarazu svjesno i namjerno neznam koju skrivenu agendu imaju ali ovaj debilizam i amaterizam njihovih takozvanih mjera sa pandemjom nema veze sa strukom nego sa politikom i kriminalom.
Guest- Guest
Re: Da remiziram...vol II.
by Guest 14/3/2021, 23:08
The EMA covid-19 data leak, and what it tells us about mRNA instability
Leaked documents show that some early commercial batches of Pfizer-BioNTech’s covid-19 vaccine had lower than expected levels of intact mRNA, prompting wider questions about how to assess this novel vaccine platform, writes Serena Tinari
As it conducted its analysis of the Pfizer-BioNTech covid-19 vaccine in December, the European Medicines Agency (EMA) was the victim of a cyberattack.1 More than 40 megabytes of classified information from the agency’s review were published on the dark web, and several journalists—including from The BMJ—and academics worldwide were sent copies of the leaks. They came from anonymous email accounts and most efforts to interact with the senders were unsuccessful. None of the senders revealed their identity, and the EMA says it is pursuing a criminal investigation.
The BMJ has reviewed the documents, which show that regulators had major concerns over unexpectedly low quantities of intact mRNA in batches of the vaccine developed for commercial production.
EMA scientists tasked with ensuring manufacturing quality—the chemistry, manufacturing, and control aspects of Pfizer’s submission to the EMA—worried about “truncated and modified mRNA species present in the finished product.” Among the many files leaked to The BMJ, an email dated 23 November by a high ranking EMA official outlined a raft of issues. In short, commercial manufacturing was not producing vaccines to the specifications expected, and regulators were unsure of the implications. EMA responded by filing two “major objections” with Pfizer, along with a host of other questions it wanted addressed.
The email identified “a significant difference in % RNA integrity/truncated species” between the clinical batches and proposed commercial batches—from around 78% to 55%. The root cause was unknown and the impact of this loss of RNA integrity on safety and efficacy of the vaccine was “yet to be defined,” the email said.
Ultimately, on 21 December, EMA authorised Pfizer-BioNTech’s vaccine. The agency’s public assessment report, a technical document published on its website, noted, “the quality of this medicinal product, submitted in the emergency context of the current (covid-19) pandemic, is considered to be sufficiently consistent and acceptable.”2
It’s unclear how the agency’s concerns were satisfied. According to one of the leaked emails dated 25 November, positive news had come from an undisclosed source in the US: “The latest lots indicate that % intact RNA are back at around 70-75%, which leaves us cautiously optimistic that additional data could address the issue,” the email said.
A near miss?
It’s also unclear whether the events in November constitute a near miss in the commercial manufacturing of mRNA vaccines.
EMA says the leaked information was partially doctored, explaining in a statement that “whilst individual emails are authentic, data from different users were selected and aggregated, screenshots from multiple folders and mailboxes have been created, and additional titles were added by the perpetrators.”3
But the documents offer the broader medical community a chance to reflect on the complexities of quality assurance for novel mRNA vaccines, which include everything from the quantification and integrity of mRNA and carrier lipids to measuring the distribution of particle sizes and encapsulation efficiency. Of particular concern is RNA instability, one of the most important variables relevant to all mRNA vaccines that has thus far received scant attention in the clinical community. It is an issue relevant not just to Pfizer-BioNTech’s vaccine but also to those produced by Moderna, CureVac, and others,4 as well as a “second generation” mRNA vaccine being pursued by Imperial College London.5
RNA instability is one of the biggest hurdles for researchers developing nucleic acid based vaccines. It is the primary reason for the technology’s stringent cold chain requirements and has been addressed by encapsulating the mRNA in lipid nanoparticles (box).
“The complete, intact mRNA molecule is essential to its potency as a vaccine,” professor of biopharmaceutics Daan J.A. Crommelin and colleagues wrote in a review article in The Journal of Pharmaceutical Sciences late last year. “Even a minor degradation reaction, anywhere along a mRNA strand, can severely slow or stop proper translation performance of that strand and thus result in the incomplete expression of the target antigen.”6
Crommelin and colleagues note that specific regulatory guidance for mRNA based vaccines has yet to be developed, and The BMJ’s attempts to clarify current standards were unsuccessful.
Transparency and confidentiality
The BMJ asked Pfizer, Moderna, and CureVac, as well as several regulators, what percentage mRNA integrity they consider acceptable for vaccines against covid-19. None offered any specifics.
The Medicines and Healthcare products Regulatory Agency, the UK’s medicines regulator, acknowledged the lack of a specified percentage RNA integrity, but declined to provide further detail. “The specification limit acceptance criteria are commercially confidential,” the agency said in an email.
The US Food and Drug Administration (FDA) directed The BMJ to read its guidance documents78 and its review of Pfizer’s vaccine,9 but none of these specify the percentage RNA the agency is requiring. Asked to comment, the regulator pointed to Pfizer: “information that you seek that is not addressed in the FDA Review Memorandum should be directed to Pfizer.”
In subsequent correspondence, FDA, EMA, and Canadian government department Health Canada all stated that specific information related to the acceptability criteria is confidential.
EMA did acknowledge, however, that vaccine efficacy depends on the presence of suitable amounts of intact mRNA. In the case of the commercial batches that first raised alarm bells, the agency told The BMJ that the levels of truncated mRNA “and the amounts of a potential protein produced by the truncated mRNA would be too low to constitute a safety risk.” EMA did not comment on how truncated mRNA might affect efficacy. The issue was satisfactorily addressed, the agency underlined, when further information was supplied by the manufacturer.
Health Canada told The BMJ that Pfizer had conducted investigations into the root cause of reduced integrity in the commercial vaccine batches, and “changes were made in their processes to ensure that the integrity was improved and brought in line with what was seen for clinical trial batches.” Health Canada said the three agencies subsequently determined that “there was no concern with the RNA integrity or any other product specifications.”
Correspondence in the leaked documents suggests that FDA, Health Canada, and EMA were aligned on clinically qualified specifications of percentage mRNA integrity. Health Canada has confirmed to The BMJ that regulators “have worked together to align those requirements,” but all agencies declined to share with The BMJ any specifics on grounds that such information was commercially sensitive.
Pfizer also declined to comment on what percentage mRNA integrity it is aiming for, nor would it address questions about the cause of the unexpectedly low percentage mRNA integrity in certain batches, leaving open the question of whether it could happen again. Pfizer stressed: “Each batch of vaccines is tested by the official medicinal control laboratory—the Paul Ehrlich Institute in Germany—before final product release. As a result, the quality of all vaccine doses that are placed on the market in Europe has been double tested to ensure compliance with the specifications agreed upon with the regulatory authorities.”
Moderna’s chief corporate affairs officer Ray Jordan declined to respond to any of The BMJ’s questions, stating: “At this point, Moderna will not be offering additional commentary on these topics.”
CureVac, whose mRNA vaccine was submitted for EMA’s “rolling review” in February,10 told The BMJ that “it is too soon to give details.”
The shortage of information may reflect the lack of certainty, even among regulators, about how to assess the evidence fully for this novel technology. Professor Crommelin told The BMJ that, “For small, low molecular weight products, the active pharmaceutical ingredient integrity is typically close to 100%.”
But for mRNA vaccines? “Experience with mRNA integrity is limited.”
Lipid nanoparticles—where do they go and what do they do?
Conceived three decades ago, RNA based therapeutics11 have long inspired imaginations for their theoretical potential to transform cells of the body into “an on-demand drug factory.”12 But despite heavy investment by the biotech industry, bench-to-bedside translation was constantly hindered by the fragility of mRNA.
Over the years, researchers attempted to resolve intrinsic instability by encapsulating mRNA in nanocarriers made of polymers, lipids, or inorganic materials. Lipid nanoparticles (LNPs) were chosen by Moderna, Pfizer-BioNTech, CureVac, and Imperial College London for their covid-19 vaccines. This has attracted the attention of specialists in the field of pharmaceutical biotechnology, some of whom have raised concerns about further unknowns.
In a rapid response posted on bmj.com, JW Ulm, a gene therapy specialist who has published on tissue targeting of therapeutic vectors,13 raised concerns about the biodistribution of LNPs: “At present, relatively little has been reported on the tissue localisation of the LNPs used to encase the SARS-CoV-2 spike protein-encoding messenger RNA, and it is vital to have more specific information on precisely where the liposomal nanoparticles are going after injection.”14
It is an unknown that Ulm worries could have implications for vaccine safety.
Ulm told The BMJ: “Pfizer-BioNTech and Moderna did a remarkable job of rapidly scaling up manufacturing of such a novel system in swift fashion, which is genuinely a landmark technological achievement. However, pharmacokinetic studies, with independent laboratory confirmation, are essential to ascertain potential cytotoxicity and macroscopic toxicity, especially given the likelihood of booster injections over months or years, since the tissue trafficking patterns of the mRNA vaccine payload will determine which cells and tissues are killed by cytotoxic T-cells in each round.” Given the variation in LNP formulations, it is unclear how relevant previous animal experiments are to answering this question.
Regulators and manufacturers contacted by The BMJ for this article did not wish to address any of the questions raised by Ulm’s rapid response.
--------------------------------------------------
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://www.bmj.com/content/372/bmj.n627
Leaked documents show that some early commercial batches of Pfizer-BioNTech’s covid-19 vaccine had lower than expected levels of intact mRNA, prompting wider questions about how to assess this novel vaccine platform, writes Serena Tinari
As it conducted its analysis of the Pfizer-BioNTech covid-19 vaccine in December, the European Medicines Agency (EMA) was the victim of a cyberattack.1 More than 40 megabytes of classified information from the agency’s review were published on the dark web, and several journalists—including from The BMJ—and academics worldwide were sent copies of the leaks. They came from anonymous email accounts and most efforts to interact with the senders were unsuccessful. None of the senders revealed their identity, and the EMA says it is pursuing a criminal investigation.
The BMJ has reviewed the documents, which show that regulators had major concerns over unexpectedly low quantities of intact mRNA in batches of the vaccine developed for commercial production.
EMA scientists tasked with ensuring manufacturing quality—the chemistry, manufacturing, and control aspects of Pfizer’s submission to the EMA—worried about “truncated and modified mRNA species present in the finished product.” Among the many files leaked to The BMJ, an email dated 23 November by a high ranking EMA official outlined a raft of issues. In short, commercial manufacturing was not producing vaccines to the specifications expected, and regulators were unsure of the implications. EMA responded by filing two “major objections” with Pfizer, along with a host of other questions it wanted addressed.
The email identified “a significant difference in % RNA integrity/truncated species” between the clinical batches and proposed commercial batches—from around 78% to 55%. The root cause was unknown and the impact of this loss of RNA integrity on safety and efficacy of the vaccine was “yet to be defined,” the email said.
Ultimately, on 21 December, EMA authorised Pfizer-BioNTech’s vaccine. The agency’s public assessment report, a technical document published on its website, noted, “the quality of this medicinal product, submitted in the emergency context of the current (covid-19) pandemic, is considered to be sufficiently consistent and acceptable.”2
It’s unclear how the agency’s concerns were satisfied. According to one of the leaked emails dated 25 November, positive news had come from an undisclosed source in the US: “The latest lots indicate that % intact RNA are back at around 70-75%, which leaves us cautiously optimistic that additional data could address the issue,” the email said.
A near miss?
It’s also unclear whether the events in November constitute a near miss in the commercial manufacturing of mRNA vaccines.
EMA says the leaked information was partially doctored, explaining in a statement that “whilst individual emails are authentic, data from different users were selected and aggregated, screenshots from multiple folders and mailboxes have been created, and additional titles were added by the perpetrators.”3
But the documents offer the broader medical community a chance to reflect on the complexities of quality assurance for novel mRNA vaccines, which include everything from the quantification and integrity of mRNA and carrier lipids to measuring the distribution of particle sizes and encapsulation efficiency. Of particular concern is RNA instability, one of the most important variables relevant to all mRNA vaccines that has thus far received scant attention in the clinical community. It is an issue relevant not just to Pfizer-BioNTech’s vaccine but also to those produced by Moderna, CureVac, and others,4 as well as a “second generation” mRNA vaccine being pursued by Imperial College London.5
RNA instability is one of the biggest hurdles for researchers developing nucleic acid based vaccines. It is the primary reason for the technology’s stringent cold chain requirements and has been addressed by encapsulating the mRNA in lipid nanoparticles (box).
“The complete, intact mRNA molecule is essential to its potency as a vaccine,” professor of biopharmaceutics Daan J.A. Crommelin and colleagues wrote in a review article in The Journal of Pharmaceutical Sciences late last year. “Even a minor degradation reaction, anywhere along a mRNA strand, can severely slow or stop proper translation performance of that strand and thus result in the incomplete expression of the target antigen.”6
Crommelin and colleagues note that specific regulatory guidance for mRNA based vaccines has yet to be developed, and The BMJ’s attempts to clarify current standards were unsuccessful.
Transparency and confidentiality
The BMJ asked Pfizer, Moderna, and CureVac, as well as several regulators, what percentage mRNA integrity they consider acceptable for vaccines against covid-19. None offered any specifics.
The Medicines and Healthcare products Regulatory Agency, the UK’s medicines regulator, acknowledged the lack of a specified percentage RNA integrity, but declined to provide further detail. “The specification limit acceptance criteria are commercially confidential,” the agency said in an email.
The US Food and Drug Administration (FDA) directed The BMJ to read its guidance documents78 and its review of Pfizer’s vaccine,9 but none of these specify the percentage RNA the agency is requiring. Asked to comment, the regulator pointed to Pfizer: “information that you seek that is not addressed in the FDA Review Memorandum should be directed to Pfizer.”
In subsequent correspondence, FDA, EMA, and Canadian government department Health Canada all stated that specific information related to the acceptability criteria is confidential.
EMA did acknowledge, however, that vaccine efficacy depends on the presence of suitable amounts of intact mRNA. In the case of the commercial batches that first raised alarm bells, the agency told The BMJ that the levels of truncated mRNA “and the amounts of a potential protein produced by the truncated mRNA would be too low to constitute a safety risk.” EMA did not comment on how truncated mRNA might affect efficacy. The issue was satisfactorily addressed, the agency underlined, when further information was supplied by the manufacturer.
Health Canada told The BMJ that Pfizer had conducted investigations into the root cause of reduced integrity in the commercial vaccine batches, and “changes were made in their processes to ensure that the integrity was improved and brought in line with what was seen for clinical trial batches.” Health Canada said the three agencies subsequently determined that “there was no concern with the RNA integrity or any other product specifications.”
Correspondence in the leaked documents suggests that FDA, Health Canada, and EMA were aligned on clinically qualified specifications of percentage mRNA integrity. Health Canada has confirmed to The BMJ that regulators “have worked together to align those requirements,” but all agencies declined to share with The BMJ any specifics on grounds that such information was commercially sensitive.
Pfizer also declined to comment on what percentage mRNA integrity it is aiming for, nor would it address questions about the cause of the unexpectedly low percentage mRNA integrity in certain batches, leaving open the question of whether it could happen again. Pfizer stressed: “Each batch of vaccines is tested by the official medicinal control laboratory—the Paul Ehrlich Institute in Germany—before final product release. As a result, the quality of all vaccine doses that are placed on the market in Europe has been double tested to ensure compliance with the specifications agreed upon with the regulatory authorities.”
Moderna’s chief corporate affairs officer Ray Jordan declined to respond to any of The BMJ’s questions, stating: “At this point, Moderna will not be offering additional commentary on these topics.”
CureVac, whose mRNA vaccine was submitted for EMA’s “rolling review” in February,10 told The BMJ that “it is too soon to give details.”
The shortage of information may reflect the lack of certainty, even among regulators, about how to assess the evidence fully for this novel technology. Professor Crommelin told The BMJ that, “For small, low molecular weight products, the active pharmaceutical ingredient integrity is typically close to 100%.”
But for mRNA vaccines? “Experience with mRNA integrity is limited.”
Lipid nanoparticles—where do they go and what do they do?
Conceived three decades ago, RNA based therapeutics11 have long inspired imaginations for their theoretical potential to transform cells of the body into “an on-demand drug factory.”12 But despite heavy investment by the biotech industry, bench-to-bedside translation was constantly hindered by the fragility of mRNA.
Over the years, researchers attempted to resolve intrinsic instability by encapsulating mRNA in nanocarriers made of polymers, lipids, or inorganic materials. Lipid nanoparticles (LNPs) were chosen by Moderna, Pfizer-BioNTech, CureVac, and Imperial College London for their covid-19 vaccines. This has attracted the attention of specialists in the field of pharmaceutical biotechnology, some of whom have raised concerns about further unknowns.
In a rapid response posted on bmj.com, JW Ulm, a gene therapy specialist who has published on tissue targeting of therapeutic vectors,13 raised concerns about the biodistribution of LNPs: “At present, relatively little has been reported on the tissue localisation of the LNPs used to encase the SARS-CoV-2 spike protein-encoding messenger RNA, and it is vital to have more specific information on precisely where the liposomal nanoparticles are going after injection.”14
It is an unknown that Ulm worries could have implications for vaccine safety.
Ulm told The BMJ: “Pfizer-BioNTech and Moderna did a remarkable job of rapidly scaling up manufacturing of such a novel system in swift fashion, which is genuinely a landmark technological achievement. However, pharmacokinetic studies, with independent laboratory confirmation, are essential to ascertain potential cytotoxicity and macroscopic toxicity, especially given the likelihood of booster injections over months or years, since the tissue trafficking patterns of the mRNA vaccine payload will determine which cells and tissues are killed by cytotoxic T-cells in each round.” Given the variation in LNP formulations, it is unclear how relevant previous animal experiments are to answering this question.
Regulators and manufacturers contacted by The BMJ for this article did not wish to address any of the questions raised by Ulm’s rapid response.
--------------------------------------------------
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://www.bmj.com/content/372/bmj.n627
Guest- Guest
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 23:27
Gnječo, imali smo u obitelji slučaj u samoizolaciji (poziotivan PCR) i nitko zbog toga nije bio pozitivan.Gnječ wrote:Eroo wrote:Gnječ wrote:evo kako sam pisao u nekoliko navrata ovo je glavni uzrok napredovanja pandemije:
ŠEF ISTARSKOG STOŽERA ZABRINUT: U Istri se virus kreće unutar obitelji zato što se ljudi ne pridržavaju samoizolacije pa se zarazi cijela obitelj. Izolirajte se od zdravih osoba oko sebe!
jebotebog kakva je to kurčeva samoizolacija u stanu okružen članovima obitelji gdje usput u posjetu dolaze i vanjski članovi uže i šire obitelji i prijatelji i susjedi !????
nekad davno su ljude oboljele od zaraznih bolesi hospitalizirali na odjel zaraznih bolesti a ovi novostvoreni današnji kreteni zaražene šalju u samoizolaciju među nezaražene pa se čude zašto pandemija nikako da stane.
https://www.glasistre.hr/istra/ff-706809
Gnječo, ako se sjećaš u par navrata sam spominjao Istru kao dobar primjer za kontrolu širenja epidemije,
a ujedno sam upozorio na mogući "zamor", jer su i istrani krvavi ispod kože. Postotak kolektivne imunizacije
je u Istri izrazito nizak, niži od bilo koje regije u Europi, ali je zato i bazen za širenje virusa s time veći.
Čak sam i predlagao da se u slučaju Istre odstupi od načela "ravnomjernog cijepljenja, u skladu sa brojem
stanovnika po županijama". Sličan primjer smo imali i u Sloveniji - Primorska.Zbog blizine Italije tamo su se
ljudi od samog početka ponašali izrazito disciplinirano. No, na kraju se popustilo i ušlo se u fazu većeg
relativno većeg širenja virusa. Tipičan primjer gdje Donnelly- Fergusonov model u jednom dijelui odkaže, a na kraju se
može u nekom smislu potvrditi. Ipak se ovdje radi o ljudima i ne kravama po farmama. Faktor koji je zbog mnogo
toga veoma teško matematički modelirati.
a bokte, jel tebi ovako kao laiku ne izgleda apsurdno i totalno van svih medicinskih protokola poslati zaražene u samoizolaciju među nezaražene ljude? i onda se debili čude da imaju porast zaraženih? kakvog smisla imaju sve te njihove kurčeve mjere i zabrane kad stožer sam generira zarazu svjesno i namjerno neznam koju skrivenu agendu imaju ali ovaj debilizam i amaterizam njihovih takozvanih mjera sa pandemjom nema veze sa strukom nego sa politikom i kriminalom.
Nismo zbog toga ni malo trpili...Jes me malo stisnilo kad su mi došli doma i samo smo razgovarali ispred
ulaza...Sin je na tome ustrajao. Odluka mu je bila sasvom na mjestu.
Sve se može, kad se male ruke slože..

Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Guest 14/3/2021, 23:39
The uncovering of the vaccination data in Israel reveals a frightening picture
14.March update: After 1 month:Israel Health Ministry 'needs more time to check' vax deaths following our Freedom of Information Act request
- answer to the 5 and 6 eugenic debunking try this time from germany and israel which bring us a table that confirm again the toxicity of the Pfizer vax.
11.March update: An other try of debunking for nakim.org and this time by Flora Teoh linked to the Sorros/Bill Gates/Carnegie eugenics network well known for spreading FAKE SCIENTIFIC NEWS through their network of paid and corrupted Fact Checkers as we will see in my answer.
10.March update:
an association of 30000 M.Ds presented our analyses for challenging the vaccination campaign in France,see report in francesoir.fr and Nexus youtube channel here.
5.March.2021 update:
we have debunked the debunkers the article of Jean-François Cliche lesoleil.com and the one of Bill Gates 'MSN network
please see our debunking in french below, and in english here.
with our conclusion: LeSoleil/Jean-François Cliche+Msn/Dan Satherley=Bill Gates=FAKE NEWS for pushing people to take the shot.
3.March.2021 update:
- this article has been published first in hebrew here
- we gave an interview in French to francesoir.fr who translated it in french here
- it has been as well reported in russian here in english in Arutz 7 here and in the U.S here
- and reported in several other language including greek here
this article can not be debunked since it is based on real data that have been exposed but since its publication the Israeli ministry of health and the Pfizer/Moderna coalition keep trying to deceive the public with biased "scientific" article (like the new england journal of medicine)that intentionally focus on the Covid sickness two weeks after the 2nd shot and hide the most important data that is the death numbers among the vaccinated people from covid and other adverse effects after the first shot.The fact that Dr Ran Balicer the corresponding author of the NEJM publication, works for the Israeli health department as head of the Klalit research institute and received grants from Pfizer may explain it...as well as 7 other co-authors of the publication.. see here
We have debunked the NEJM study please read our article, their datas validate our analysis and show 3 time increase of Covid19 after first shot, here:
Exposing distortions in the NEJM scientific publication on the efficiency of Pfizer's vax
The uncovering of the vaccination data in Israel reveals a frightening picture
Analyses below of an article promoting COVID-19 vaccination enable to uncover all vaccination data and a frightening situation
Second draft
On February 11 2021 Ynet (the most known Israeli News website) published a confused and confusing article entitled "Vaccination efficiency data in Israel, and its rapid effects on the young".
Our reanalyses of these data explain why during the massive vaccination project initiated mid-December 2020 during a confinement, daily new confirmed COVID-19 cases failed to decrease as they do during confinements, and, more importantly, why numbers of serious, critical and death cases increased during that period that covered at least one month. From mid-December to mid-February (two months), 2337 among all Israeli 5351 official COVID-deaths occurred.Our analyses indicate orders of magnitude increases in deaths rates during the 5-week long vaccination process, as compared to the unvaccinated and those after completing the vaccination process. Presumably, asymptomatic cases before vaccination, and those infected shortly after the 1st dose, tend to develop graver symptoms than those unvaccinated.
The Ynet article is organised in an exciting way and uses data provided in an erroneous way by the Ministry of Health. It is unclear whether this was intentional to prove the vaccine's efficiency or if this was done erroneously because the provided data were misunderstood.Note that in Israel, all vaccines are from Pfizer.
We bring a very important example from the article, in relation to the table provided by the Ministry of Health. As per the text "However, 546 among the dead were such that were not at all vaccinated or got the first vaccination dose within two weeks before their death" differs from the table. This is clearly unfounded because all data presented in the table and provided below describe only COVID-19 patients that got at least the first vaccination dose. This is clear from examining the table. The grand total is 43781 COVID patients who got the first or the second vaccine dose. Among the total of 660 deaths, 546 got only the first dose.
The data in the table, rather than indicating the vaccine efficiency, indicate the vaccine's adverse effects.
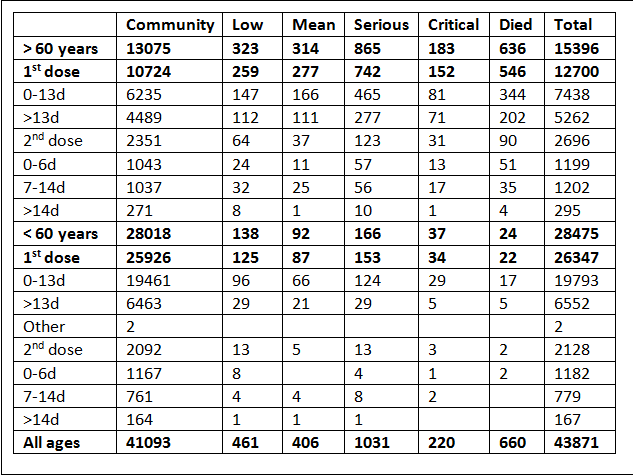
For that purpose we need first to understand that the provided table describes the state of COVID-19 patients that got the first or the second vaccine dose at given dates, as started in the article "…emerges from the data that among 856 patients above 60 years in serious state hospitalized at this time…" we assume that the article published February 11 reflects the situation in hospitals the previous day, hence February 10 2021, or February 11 2021.
On February 10, the number of serious active cases was 1056 according to the control panel of the Ministry of Health, see photo below.
This surprisingly shows that most serious hospitalized cases on February 10 or at a near date were in fact vaccinated with the first dose or up to two weeks after the second dose. See the table of the vaccinated patients showing 1031 serious and 220 critical cases at the time the table was done. This matches the article in hebrew from February 1st 2021 "Can one show that the vaccine from Pfizer is today's major cause for high death rates in Israel and the world?".
However, this is not the last surprise we get from examining the data from the Ministry of Health.
We can substract the number of people with the first vaccine dose on January 19 2021 from that on February 10 2021. During these 21 days, 1331881 Israeli citizens got the first dose. The table shows that 568 among these died, hence 0.042% and that 39047 among them became a COVID-19 case, hence 2.9 %.
For the 2nd dose we focus on data specific to two weeks after the 2nd vaccination according to the table.
From January 26 to February 10 2021 909102 Israeli citizens got the 2nd vaccine dose. Among these according to the table, 92 died, 0.01%.
Hence, during the 5 weeks since the first dose at least 0.05% of first dose recipients died. This death rate relates mainly to a relatively young population whose vaccination stated on January 19, a period during which most vaccinated were below 65.
In order to estimate the death rate of those above 65 which were mostly vaccinated before that period we use data reported by the USA-based VAERS,
There we found, see article in english, that the ratio of deaths by those above 65 vs those below 65 is about 4.42 (155/35). Hence the death rate of those above 65 between the first and the second vaccination dose should be until January 19 0.042 (the death rate of those below 65) multiplied by 4.42, resulting in 0.186%, which is close to the 0.2% reported by the Ministry of Health on January 21 2021.
This value of 0.2 % death has been mysteriously modified later on by the Ministry of Health and was switched to 0.005 without any explanation, see article in hebrew. Above considerations show that the death rate data provided first were correct, the updated death rate data might have been intended to suggest lower death rates among the elderly.
The exposures do not end here.
The number of COVID-19 deaths among the vaccinated since the start of the vaccination action seems to explain the increased death rates from COVID-19 observed since December 2020.
For that purpose, we calculate the products of the number of vaccinated people above age 65 by 0.2 and the number of vaccinated people below 65 by 0.04. This shows that most COVID-19 deaths in that period are for vaccinated people, as shows the table provided by the Ministry of health at the beginning of February.
During the vaccination action from mid-December until mid-February, 2337 among all 5351 COVID-19 deaths reported for Israel occurred, 43.7%. Among these, since January 19, 1271 COVID-19 deaths were reported for Israel.The table provided by the Ministry of Health on February 10 states 660 COVID-19 deaths among the vaccinated, 51.9% of the deaths for that period. Only 1.3 million Israeli, among 8 million (about 1 in 8, 12.5%), were vaccinated during that period. Accordingly, vaccination promotes deaths because 51.9% of deaths during that period are for the 12.5% vaccinated in that period. In addition the serious and critical cases during that period is more than the reported serious cases, the adverse effect of the vaccination process is most likely worse than what appears from the data at hand.
The horror continues. The deaths among those vaccinated should be added to the numerous AVC and cardiac events reported just after vaccination that are not included among COVID-19 deaths which about double the deaths among those vaccinated, whose numbers remain unknown and which we will try to find in the coming days.
At this point we state that vaccinations caused more deaths than the coronavirus would have during the same period.
Among those vaccinated and above 65, 0.2% of those vaccinated died during the 3-week period between doses, hence about 200 among 100000 vaccinated. This is to be compared to the 4.91 dead among 100000 dying from COVID-19 without vaccination, see below. This should not be confused with the COVID-19 0.279 deaths among 100000 reported for those who completed the vaccination process, meaning 2 weeks after the second dose, see below table from the Ynet article.
14.March update: After 1 month:Israel Health Ministry 'needs more time to check' vax deaths following our Freedom of Information Act request
- answer to the 5 and 6 eugenic debunking try this time from germany and israel which bring us a table that confirm again the toxicity of the Pfizer vax.
11.March update: An other try of debunking for nakim.org and this time by Flora Teoh linked to the Sorros/Bill Gates/Carnegie eugenics network well known for spreading FAKE SCIENTIFIC NEWS through their network of paid and corrupted Fact Checkers as we will see in my answer.
10.March update:
an association of 30000 M.Ds presented our analyses for challenging the vaccination campaign in France,see report in francesoir.fr and Nexus youtube channel here.
5.March.2021 update:
we have debunked the debunkers the article of Jean-François Cliche lesoleil.com and the one of Bill Gates 'MSN network
please see our debunking in french below, and in english here.
with our conclusion: LeSoleil/Jean-François Cliche+Msn/Dan Satherley=Bill Gates=FAKE NEWS for pushing people to take the shot.
3.March.2021 update:
- this article has been published first in hebrew here
- we gave an interview in French to francesoir.fr who translated it in french here
- it has been as well reported in russian here in english in Arutz 7 here and in the U.S here
- and reported in several other language including greek here
this article can not be debunked since it is based on real data that have been exposed but since its publication the Israeli ministry of health and the Pfizer/Moderna coalition keep trying to deceive the public with biased "scientific" article (like the new england journal of medicine)that intentionally focus on the Covid sickness two weeks after the 2nd shot and hide the most important data that is the death numbers among the vaccinated people from covid and other adverse effects after the first shot.The fact that Dr Ran Balicer the corresponding author of the NEJM publication, works for the Israeli health department as head of the Klalit research institute and received grants from Pfizer may explain it...as well as 7 other co-authors of the publication.. see here
We have debunked the NEJM study please read our article, their datas validate our analysis and show 3 time increase of Covid19 after first shot, here:
Exposing distortions in the NEJM scientific publication on the efficiency of Pfizer's vax
The uncovering of the vaccination data in Israel reveals a frightening picture
Analyses below of an article promoting COVID-19 vaccination enable to uncover all vaccination data and a frightening situation
Second draft
On February 11 2021 Ynet (the most known Israeli News website) published a confused and confusing article entitled "Vaccination efficiency data in Israel, and its rapid effects on the young".
Our reanalyses of these data explain why during the massive vaccination project initiated mid-December 2020 during a confinement, daily new confirmed COVID-19 cases failed to decrease as they do during confinements, and, more importantly, why numbers of serious, critical and death cases increased during that period that covered at least one month. From mid-December to mid-February (two months), 2337 among all Israeli 5351 official COVID-deaths occurred.Our analyses indicate orders of magnitude increases in deaths rates during the 5-week long vaccination process, as compared to the unvaccinated and those after completing the vaccination process. Presumably, asymptomatic cases before vaccination, and those infected shortly after the 1st dose, tend to develop graver symptoms than those unvaccinated.
The Ynet article is organised in an exciting way and uses data provided in an erroneous way by the Ministry of Health. It is unclear whether this was intentional to prove the vaccine's efficiency or if this was done erroneously because the provided data were misunderstood.Note that in Israel, all vaccines are from Pfizer.
We bring a very important example from the article, in relation to the table provided by the Ministry of Health. As per the text "However, 546 among the dead were such that were not at all vaccinated or got the first vaccination dose within two weeks before their death" differs from the table. This is clearly unfounded because all data presented in the table and provided below describe only COVID-19 patients that got at least the first vaccination dose. This is clear from examining the table. The grand total is 43781 COVID patients who got the first or the second vaccine dose. Among the total of 660 deaths, 546 got only the first dose.
The data in the table, rather than indicating the vaccine efficiency, indicate the vaccine's adverse effects.

For that purpose we need first to understand that the provided table describes the state of COVID-19 patients that got the first or the second vaccine dose at given dates, as started in the article "…emerges from the data that among 856 patients above 60 years in serious state hospitalized at this time…" we assume that the article published February 11 reflects the situation in hospitals the previous day, hence February 10 2021, or February 11 2021.
On February 10, the number of serious active cases was 1056 according to the control panel of the Ministry of Health, see photo below.
This surprisingly shows that most serious hospitalized cases on February 10 or at a near date were in fact vaccinated with the first dose or up to two weeks after the second dose. See the table of the vaccinated patients showing 1031 serious and 220 critical cases at the time the table was done. This matches the article in hebrew from February 1st 2021 "Can one show that the vaccine from Pfizer is today's major cause for high death rates in Israel and the world?".
However, this is not the last surprise we get from examining the data from the Ministry of Health.
We can substract the number of people with the first vaccine dose on January 19 2021 from that on February 10 2021. During these 21 days, 1331881 Israeli citizens got the first dose. The table shows that 568 among these died, hence 0.042% and that 39047 among them became a COVID-19 case, hence 2.9 %.
For the 2nd dose we focus on data specific to two weeks after the 2nd vaccination according to the table.
From January 26 to February 10 2021 909102 Israeli citizens got the 2nd vaccine dose. Among these according to the table, 92 died, 0.01%.
Hence, during the 5 weeks since the first dose at least 0.05% of first dose recipients died. This death rate relates mainly to a relatively young population whose vaccination stated on January 19, a period during which most vaccinated were below 65.
In order to estimate the death rate of those above 65 which were mostly vaccinated before that period we use data reported by the USA-based VAERS,
There we found, see article in english, that the ratio of deaths by those above 65 vs those below 65 is about 4.42 (155/35). Hence the death rate of those above 65 between the first and the second vaccination dose should be until January 19 0.042 (the death rate of those below 65) multiplied by 4.42, resulting in 0.186%, which is close to the 0.2% reported by the Ministry of Health on January 21 2021.
This value of 0.2 % death has been mysteriously modified later on by the Ministry of Health and was switched to 0.005 without any explanation, see article in hebrew. Above considerations show that the death rate data provided first were correct, the updated death rate data might have been intended to suggest lower death rates among the elderly.
The exposures do not end here.
The number of COVID-19 deaths among the vaccinated since the start of the vaccination action seems to explain the increased death rates from COVID-19 observed since December 2020.
For that purpose, we calculate the products of the number of vaccinated people above age 65 by 0.2 and the number of vaccinated people below 65 by 0.04. This shows that most COVID-19 deaths in that period are for vaccinated people, as shows the table provided by the Ministry of health at the beginning of February.
During the vaccination action from mid-December until mid-February, 2337 among all 5351 COVID-19 deaths reported for Israel occurred, 43.7%. Among these, since January 19, 1271 COVID-19 deaths were reported for Israel.The table provided by the Ministry of Health on February 10 states 660 COVID-19 deaths among the vaccinated, 51.9% of the deaths for that period. Only 1.3 million Israeli, among 8 million (about 1 in 8, 12.5%), were vaccinated during that period. Accordingly, vaccination promotes deaths because 51.9% of deaths during that period are for the 12.5% vaccinated in that period. In addition the serious and critical cases during that period is more than the reported serious cases, the adverse effect of the vaccination process is most likely worse than what appears from the data at hand.
The horror continues. The deaths among those vaccinated should be added to the numerous AVC and cardiac events reported just after vaccination that are not included among COVID-19 deaths which about double the deaths among those vaccinated, whose numbers remain unknown and which we will try to find in the coming days.
At this point we state that vaccinations caused more deaths than the coronavirus would have during the same period.
Among those vaccinated and above 65, 0.2% of those vaccinated died during the 3-week period between doses, hence about 200 among 100000 vaccinated. This is to be compared to the 4.91 dead among 100000 dying from COVID-19 without vaccination, see below. This should not be confused with the COVID-19 0.279 deaths among 100000 reported for those who completed the vaccination process, meaning 2 weeks after the second dose, see below table from the Ynet article.
Guest- Guest
Re: Da remiziram...vol II.
by Eroo 14/3/2021, 23:54
Gnječo, ako ti se da de ovaj zadnji link "prevedi" svojim riječima na nekoliko ključnih zaključaka. Članak se mi čini veoma zanimljiv, ali sam već preumoran za ispratiti ga dovoljno koncentrirano. Za uslugu ti šaljem set od 5 brnjica.Nerabljene, garant!
_________________
Nulla rosa sine spina
Eroo- Posts : 78946
2016-07-22
Re: Da remiziram...vol II.
by Guest 14/3/2021, 23:57
This scary picture also extends to those below 65, among which, for the 5 weeks during the complete vaccination process 0.05%, meaning 50 among 100000, died. This is to be compared to the 0.19 per 100000 dying from COVID-19 and that are not vaccinated in that age group, as per the above table. Hence the death rate of this age group increased by 260 during this 5-week period of the vaccination process, as compared to their natural COVID-19 death rate.
A simple way to pass these points across relate to the monthly COVID-19 deaths rates since the start of the pandemic and until mid-December, 3014 deaths, hence 3014/9 = 334.9 deaths per month. Monthly death rates since mid-December are 2337/2 = 1168.5 deaths per month, hence 3.5 times greater.
We conclude that the Pfizer vaccines, for the elderly, killed during the 5-week vaccination period about 40 times more people than the disease itself would have killed, and about 260 times more people than the disease among the younger age class. We stress that this is in order to produce a green passport valid at most 6 months, and promote Pfizer sales.
These estimated numbers of deaths from the vaccine are probably much lower than actual numbers as it accounts only for those defined as COVID-19 deaths for that short time period and does not include AVC and cardiac (and other) events resulting from the inflammatory reactions in tens of reports documented on the NAKIM site, which themselves are only the iceberg's tip, see here.
This does not account for long-term complications described in a criminal complaint filed in December 2020 in France and which was translated to english, see here.
Looking back, this explains why the serious COVID-19 cases increased as vaccination started, and why cases started to decline when vaccination was opened to the young and continue to decline as the vaccination national campaign is losing its momentum.
We hope that this massacre will not include those below 13, as these have an increased adverse reaction rate, including death, to vaccines as shown by multi-decennial data from the VAERS reports in the USA.
We summarise that the pandemic may be predicted for the coming weeks. The decrease in vaccinations and in vaccination age will cause a decrease in serious cases, mainly not because of the protection by the vaccine, but because fewer people will die from the vaccine and other adverse vaccine reactions.
This will be temporary as in a few months we expect to face mid- and long-term adverse effects of the vaccination as ADE (Antibody-dependent Enhancement) and the vaccination-resistant mutants selected by the vaccines. But this should occur after the soon coming elections and the (survivor) voters won’t have another opportunity to express their disappointment at the voting poll.
Thanks to Dr Hervé Seligmann for his huge support on data analysis.
Haim Yativ
https://www.nakim.org/israel-forums/viewtopic.php?p=276314
A simple way to pass these points across relate to the monthly COVID-19 deaths rates since the start of the pandemic and until mid-December, 3014 deaths, hence 3014/9 = 334.9 deaths per month. Monthly death rates since mid-December are 2337/2 = 1168.5 deaths per month, hence 3.5 times greater.
We conclude that the Pfizer vaccines, for the elderly, killed during the 5-week vaccination period about 40 times more people than the disease itself would have killed, and about 260 times more people than the disease among the younger age class. We stress that this is in order to produce a green passport valid at most 6 months, and promote Pfizer sales.
These estimated numbers of deaths from the vaccine are probably much lower than actual numbers as it accounts only for those defined as COVID-19 deaths for that short time period and does not include AVC and cardiac (and other) events resulting from the inflammatory reactions in tens of reports documented on the NAKIM site, which themselves are only the iceberg's tip, see here.
This does not account for long-term complications described in a criminal complaint filed in December 2020 in France and which was translated to english, see here.
Looking back, this explains why the serious COVID-19 cases increased as vaccination started, and why cases started to decline when vaccination was opened to the young and continue to decline as the vaccination national campaign is losing its momentum.
We hope that this massacre will not include those below 13, as these have an increased adverse reaction rate, including death, to vaccines as shown by multi-decennial data from the VAERS reports in the USA.
We summarise that the pandemic may be predicted for the coming weeks. The decrease in vaccinations and in vaccination age will cause a decrease in serious cases, mainly not because of the protection by the vaccine, but because fewer people will die from the vaccine and other adverse vaccine reactions.
This will be temporary as in a few months we expect to face mid- and long-term adverse effects of the vaccination as ADE (Antibody-dependent Enhancement) and the vaccination-resistant mutants selected by the vaccines. But this should occur after the soon coming elections and the (survivor) voters won’t have another opportunity to express their disappointment at the voting poll.
Thanks to Dr Hervé Seligmann for his huge support on data analysis.
Haim Yativ
https://www.nakim.org/israel-forums/viewtopic.php?p=276314
Guest- Guest
Re: Da remiziram...vol II.
by Guest 15/3/2021, 00:08
Eroo wrote:Gnječo, ako ti se da de ovaj zadnji link "prevedi" svojim riječima na nekoliko ključnih zaključaka. Članak se mi čini veoma zanimljiv, ali sam već preumoran za ispratiti ga dovoljno koncentrirano. Za uslugu ti šaljem set od 5 brnjica.Nerabljene, garant!
ti voliš da ti se crta? grafikoni i statistika pa evo:
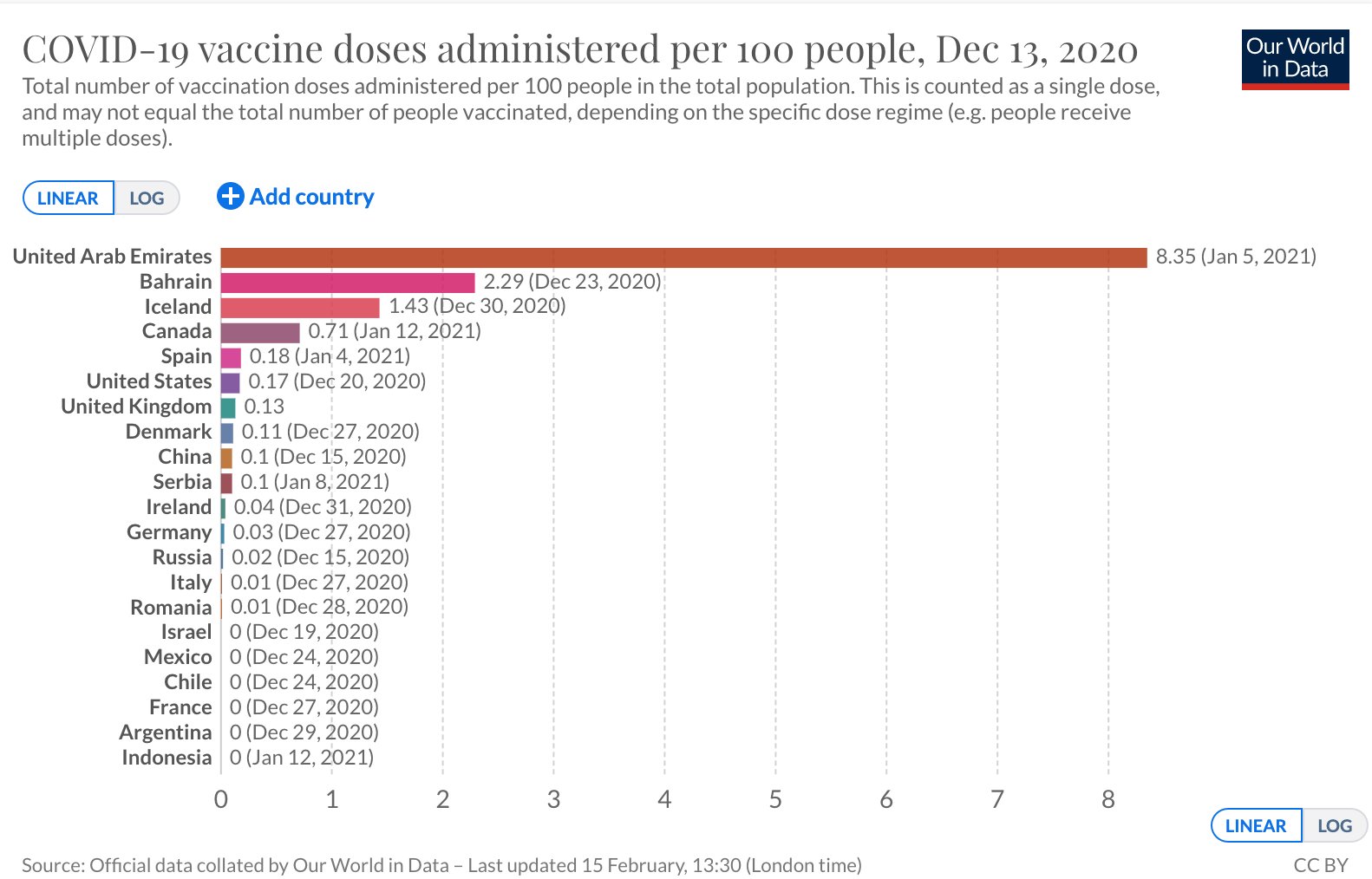
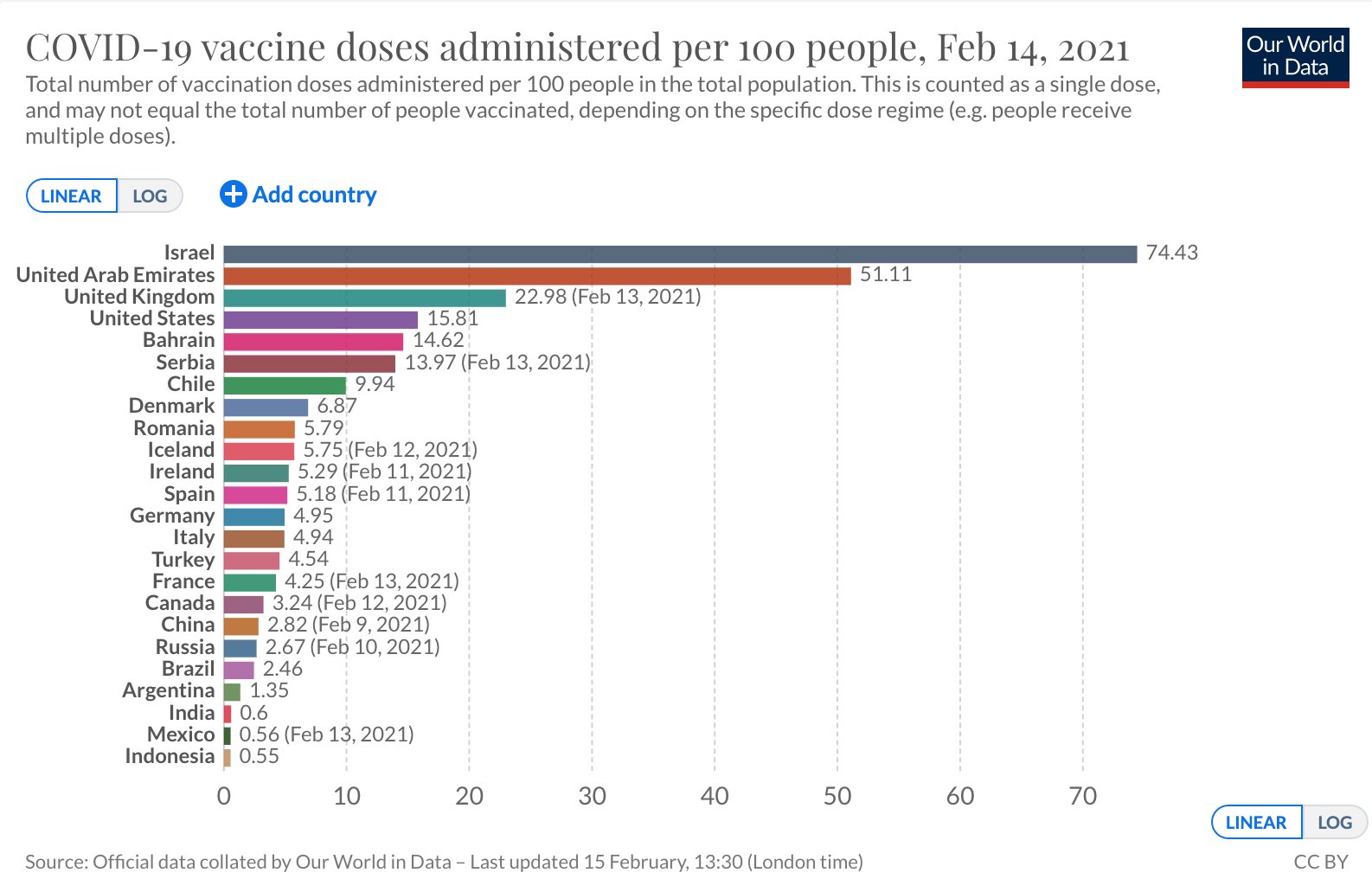
Guest- Guest
Page 13 of 50 • 1 ... 8 ... 12, 13, 14 ... 31 ... 50 ![]()
Page 13 of 50
Permissions in this forum:
You cannot reply to topics in this forum