
 Events
Events Latest images
Latest imagesKorona novosti i spoznaje
Page 27 of 50
Page 27 of 50 •  1 ... 15 ... 26, 27, 28 ... 38 ... 50
1 ... 15 ... 26, 27, 28 ... 38 ... 50 ![]()

Re: Korona novosti i spoznaje
 by Guest 24/10/2021, 18:34
by Guest 24/10/2021, 18:34
Eroo wrote:violator wrote:
Moj je primjer analogan iznesenim Tatjaninim informacijama. Ona nije spomenula koliki postotak pozitivnih otpada na necijepljene, vec koliki se postotak necijepljenih nalazi medju preminulima...
Ne sumnjam u napisano.
No,čemu služi taj podatak? Kao dokaz da je više umrlih cijepljenih nego necijepljenih?
ŽeMska glavo, zamisli ovo, ako ne bi bilo necijepljenih svi umrli bi bili cijepljeni.
Tatjana ima pred sobom 15 umrlih cijepljenih i 10 umrlih necijepljenih i ništa drugo nije rekla.
Nije tvrdila da je među cijepljenima veća smrtnost od one među necijepljenima.
Ovaj bi podatak imao smisla, a onaj prvi ne služi ničemu.
HZJZ je neki dan objavio kompletne rezultate cijepljenih i necijepljenih, kao i broj umrlih iz obe skupine.
Moja računska procjena je bila da je smrtnost među nezaštićenima 13.3x veća od one među zaštićenima.
Ovaj podatak ima smisla, jer tada epidemiolog zna što činiti kako bi smanjio smrtnost, pa i širenje zaraze,
odnosno hospitalizacije -zatrpanost zdravstvenih ustanova covid bolesnicima i tako ostavio prostor
za primarnu zaštitu. To je sve što treba znati o ovome.
Ti se meni malo gubis, Ero. :(
Gle, sve je pocelo od toga kad sam te upitala da mi pojasnis kako te to Noorka pokusala izmanipulirati jer ti je postavila jednostavno pitanje koje je pratilo Tatjanine informacije.
Onda si mi naveo primjer s vocnjakom koji nije pratio Tajinu iznesenu situaciju pa sam modificirala tvoj analogni primjer s vocnjakom i vockama (plodovima).
Kruske su necijepljeni. Ne-kruske su cijepljeni (mendule, kesteni, jabuke) jer ne znamo odnose li se na cijepljene s jednom dozom, dvije ili tri (booster).
Dakle, ja u svojem primjeru nisam tvrdila da je medju preminulima vise cijepljenih jer to nije rekla ni Tatjana.
Ovdje cu stati. Nema mi smisla ovo dalje pojasnjavati.
Guest- Guest

Re: Korona novosti i spoznaje
by Guest 24/10/2021, 18:38
Eroo wrote:Bez potrbnih ulaznih podataka nema nikakve matematike, pa čak ni one najednostavnije.Gnječ wrote:Eroo wrote:Kao prvo, uz sav respekt do doktora, ne znači da su doktori i matematički obrazovani.Gnječ wrote:
BECERRA GETS BURNED BY SEN. RAND PAUL - HRVATSKI PRIJEVOD
Senator dr. Rand Paul oštro i argumentirano kritizira bahati i podcjenjivački pristup tajnika HHS-a Xaviera Becerre (koji uopće nije liječnik nego odvjetnik) po pitanju učinkovitosti prirodno stečenog imuniteta onih koji su preboljeli COVID-19.
01.10.2021.
Prevela: Marina Čečura
Primjer Hrvatske: Držim se vaše domaće situacije,a to je ono šta bi vas moralo najviše zanimati.
Imate ukupni broj cijepljenih, kao i ukupni broj zaraženih + procjenu (često citirani Bakić, Lauc) "zamračenih" zaraženih.
Taj broj ja označavam kao "Zaštićeni", a ostali su necijepljeni, odnosno "Nezaštićeni".
Dalje, u zadnje vrijeme je HZJ par puta objavio 7 dnevne kompletne rezultate broja zaraze i broja umrlih po naznačenim skupinama.
Jednostavnim izračunom se pokazalo da je zaraženost među "Nezaštićenima" cca 10x veća, a smrtnost cca 13x veća od one
koju imate među "Zaštićenima".
Jednostavno ka pasulj.
Jebote jedan od primarnih predmeta epidemiologa je matematika. Jel si ti ikad vidio te izracune da ti pamet stane. Ti nam tu nisi dogurao dalje od tablice mnozenja i jos se oholo bahatis.
On oštro krizira, ali za ono šta iznosi nema podataka, jer ih ne može ni imati.
Znanstvene kritike na javnoj TV nije od pomoći za znanost.
Zna se kako se čini znanost.
Gnječo, prije sam ti naglasio s kojim brojevima možemo danas operirati kad je ova epidemija
u pitanju. Raspravljati javno o eventualnmi negativnim učincima u nekoj dalekoj budućnosti,
je za mene, milo rečeno, veoma upitno. U svakom slučaju je beskorisno u datom vremenu.
ti si indoktrinirani polupismeni moron. End of story.

Guest- Guest
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 18:45
Nije rekla, ali je ono šta je rekla pogrešno informirala javnost.violator wrote:Dakle, ja u svojem primjeru nisam tvrdila da je medju preminulima vise cijepljenih jer to nije rekla ni Tatjana.
Ovdje cu stati. Nema mi smisla ovo dalje pojasnjavati.
Ja sumnjam da je rekla da je cijepljenje bez veze, jer, vidite da je veći procenat cijepljenih.
Tako su njenu javnu izjavu iskoristili ravnozemlješi, jedni namjerno drugi iz neznanja.
Kamera zna ljude blokirati, pa mnogi izgube koncentarciju i lupnu svašta...
Ja sam se samo potrudio objasniti šta "Tatjaninoj" izjavi nedostaje....
Inače mi je o svemu ovome suvišno raspravljati.
Last edited by Eroo on 24/10/2021, 18:47; edited 1 time in total
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 18:46
Najnovije vijesti iz "balona"...Gnječ wrote:Eroo wrote:Bez potrbnih ulaznih podataka nema nikakve matematike, pa čak ni one najednostavnije.Gnječ wrote:Eroo wrote:Kao prvo, uz sav respekt do doktora, ne znači da su doktori i matematički obrazovani.Gnječ wrote:
BECERRA GETS BURNED BY SEN. RAND PAUL - HRVATSKI PRIJEVOD
Senator dr. Rand Paul oštro i argumentirano kritizira bahati i podcjenjivački pristup tajnika HHS-a Xaviera Becerre (koji uopće nije liječnik nego odvjetnik) po pitanju učinkovitosti prirodno stečenog imuniteta onih koji su preboljeli COVID-19.
01.10.2021.
Prevela: Marina Čečura
Primjer Hrvatske: Držim se vaše domaće situacije,a to je ono šta bi vas moralo najviše zanimati.
Imate ukupni broj cijepljenih, kao i ukupni broj zaraženih + procjenu (često citirani Bakić, Lauc) "zamračenih" zaraženih.
Taj broj ja označavam kao "Zaštićeni", a ostali su necijepljeni, odnosno "Nezaštićeni".
Dalje, u zadnje vrijeme je HZJ par puta objavio 7 dnevne kompletne rezultate broja zaraze i broja umrlih po naznačenim skupinama.
Jednostavnim izračunom se pokazalo da je zaraženost među "Nezaštićenima" cca 10x veća, a smrtnost cca 13x veća od one
koju imate među "Zaštićenima".
Jednostavno ka pasulj.
Jebote jedan od primarnih predmeta epidemiologa je matematika. Jel si ti ikad vidio te izracune da ti pamet stane. Ti nam tu nisi dogurao dalje od tablice mnozenja i jos se oholo bahatis.
On oštro krizira, ali za ono šta iznosi nema podataka, jer ih ne može ni imati.
Znanstvene kritike na javnoj TV nije od pomoći za znanost.
Zna se kako se čini znanost.
Gnječo, prije sam ti naglasio s kojim brojevima možemo danas operirati kad je ova epidemija
u pitanju. Raspravljati javno o eventualnmi negativnim učincima u nekoj dalekoj budućnosti,
je za mene, milo rečeno, veoma upitno. U svakom slučaju je beskorisno u datom vremenu.
ti si indoktrinirani polupismeni moron. End of story.
![:]](/users/3113/42/81/98/smiles/1823623843.gif)
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Guest 24/10/2021, 18:57
COVID-19 Pathophysiology and Treatments:
COVID-19 is not a viral pneumonia. It is a viral vascular endotheliitis and attacks the lining of blood vessels, particularly the small pulmonary alveolar capillaries, leading to endothelial cell activation and sloughing, coagulopathy, sepsis, pulmonary edema, and ARDS-like symptoms. This is a disease of the blood and blood vessels. The circulatory system. Any pneumonia that it causes is secondary to that.In severe cases, this leads to sepsis, blood clots, and multiple organ failure, including hypoxic and inflammatory damage to various vital organs, such as the brain, heart, liver, pancreas, kidneys, and intestines.Some of the most common laboratory findings in COVID-19 are elevated D-dimer, elevated prothrombin time, elevated C-reactive protein, neutrophilia, lymphopenia, hypocalcemia, and hyperferritinemia, essentially matching a profile of coagulopathy and immune system hyperactivation/immune cell exhaustion.COVID-19 can present as almost anything, due to the wide tropism of SARS-CoV-2 for various tissues in the body’s vital organs.
While its most common initial presentation is respiratory illness and flu-like symptoms, it can present as brain inflammation, gastrointestinal disease, or even heart attack or pulmonary embolism.COVID-19 is more severe in those with specific comorbidities, such as obesity, diabetes, and hypertension. This is because these conditions involve endothelial dysfunction, which renders the circulatory system more susceptible to infection and injury by this particular virus. The vast majority of COVID-19 cases are mild and do not cause significant disease. In known cases, there is something known as the 80/20 rule, where 80% of cases are mild and 20% are severe or critical. However, this ratio is only correct for known cases, not all infections. The number of actual infections is much, much higher. Consequently, the mortality and morbidity rate is lower. However, COVID-19 spreads very quickly, meaning that there are a significant number of severely-ill and critically-ill patientsappearing in a short time frame.In those who have critical COVID-19-induced sepsis, hypoxia, coagulopathy, and ARDS, the most common treatments are intubation, injected corticosteroids, and blood thinners. This is not the correct treatment for COVID-19. In severe hypoxia, cellular metabolic shifts cause ATP to break down into hypoxanthine, which, upon the reintroduction of oxygen, causes xanthine oxidase to produce tons of highly damaging radicals that attack tissue. This is called ischemia-reperfusion injury, and it’s why the majority of people who go on a ventilator are dying. In the mitochondria, succinate buildup due to sepsis does the same exact thing; when oxygen is reintroduced, it makes superoxide radicals. Make no mistake,intubation will kill people who have COVID-19.
The end-stage of COVID-19 is severe lipid peroxidation, where fats in the body start to “rust” due to damage by oxidative stress. This drives autoimmunity. Oxidized lipids appear as foreign objects to the immune system, which recognizes and forms antibodies against OSEs, or oxidation-specific epitopes. Also, oxidized lipids feed directly into pattern recognition receptors, triggering even more inflammation and summoning even more cells of the innate immune system that release even more destructive enzymes.
This is similar to the pathophysiology of Lupus. COVID-19’s pathology is dominated by extreme oxidative stress and neutrophil respiratory burst, to the point where hemoglobin becomes incapable of carrying oxygen due to heme iron being stripped out of heme by hypochlorous acid. No amount of supplemental oxygen can oxygenate blood that chemically refuses to bind O2.The breakdown of the pathology is as follows:SARS-CoV-2 Spike binds to ACE2. Angiotensin Converting Enzyme 2 is an enzyme that is part of the renin-angiotensin-aldosterone system, or RAAS. The RAAS is a hormone control system that moderates fluid volume in the body and in the bloodstream (i.e. osmolarity) by controlling salt retention and excretion.
This protein, ACE2, is ubiquitous in every part of the body that interfaces with the circulatory system, particularly in vascular endothelial cells and pericytes, brain astrocytes, renal tubules and podocytes, pancreatic islet cells, bile duct and intestinal epithelial cells, and the seminiferous ducts of the testis, all of which SARS-CoV-2 can infect, not just the lungs.SARS-CoV-2 infects a cell as follows: SARS-CoV-2 Spike undergoes a conformational change where the S1 trimers flip up and extend, locking onto ACE2 bound to the surface of a cell. TMPRSS2, or transmembrane protease serine 2, comes along and cuts off the heads of the Spike, exposing the S2 stalk-shaped subunit inside. The remainder of the Spike undergoes a conformational change that causes it to unfold like an extension ladder, embedding itself in the cell membrane.
Then, it folds back upon itself, pulling the viral membrane and the cell membrane together. The two membranes fuse, with the virus’s proteins migrating out onto the surface of the cell. The SARS-CoV-2 nucleocapsid enters the cell, disgorging its genetic material and beginning the viral replication process, hijacking the cell’s own structures to produce more virus.SARS-CoV-2 Spike proteins embedded in a cell can actually cause human cells to fuse together, forming syncytia/MGCs (multinuclear giant cells). They also have other pathogenic, harmful effects. SARS-CoV-2’s viroporins, such as its Envelope protein, act as calcium ion channels, introducing calcium into infected cells. The virus suppresses the natural interferon response, resulting in delayed inflammation. SARS-CoV-2 N protein can also directly activate the NLRP3 inflammasome. Also, it suppresses the Nrf2 antioxidant pathway. The suppression of ACE2 by binding with Spike causes a buildup of bradykinin that would otherwise be broken down by ACE2.
This constant calcium influx into the cells results in (or is accompanied by) noticeable hypocalcemia, or low blood calcium, especially in people with Vitamin D deficiencies and pre-existing endothelial dysfunction. Bradykinin upregulates cAMP, cGMP, COX, and Phospholipase C activity. This results inprostaglandin release and vastly increased intracellular calcium signaling, which promotes highly aggressive ROS release and ATP depletion. NADPH oxidase releases superoxide into the extracellular space. Superoxide radicals react with nitric oxide to form peroxynitrite. Peroxynitrite reacts with the tetrahydrobiopterin cofactor needed by endothelial nitric oxide synthase, destroying it and “uncoupling” the enzymes, causing nitric oxide synthase to synthesize more superoxide instead.
This proceeds in a positive feedback loop until nitric oxide bioavailability in the circulatory system is depleted. Dissolved nitric oxide gas produced constantly by eNOS serves many important functions, but it is also antiviral against SARS-like coronaviruses, preventing the palmitoylation of the viral Spike protein and making it harder for it to bind to host receptors. The loss of NO allows the virus to begin replicating with impunity in the body. Those with endothelial dysfunction (i.e. hypertension, diabetes, obesity, old age, African-American race) have redox equilibrium issues to begin with, giving the virus an advantage.Due to the extreme cytokine release triggered by these processes, the body summons a great deal of neutrophils and monocyte-derived alveolar macrophages to the lungs.
Cells of the innate immune system are the first-line defenders against pathogens. They work by engulfing invaders and trying to attack them with enzymes that produce powerful oxidants, like SOD and MPO. Superoxide dismutase takes superoxide and makes hydrogen peroxide, and myeloperoxidase takes hydrogen peroxide and chlorine ions and makes hypochlorous acid, which is many, many times more reactive than sodium hypochlorite bleach.Neutrophils have a nasty trick. They can also eject these enzymes into the extracellular space, where they will continuously spit out peroxide and bleach into the bloodstream. This is called neutrophil extracellular trap formation, or, when it becomes pathogenic and counterproductive, NETosis. In severe and critical COVID-19, there is actually rather severe NETosis.Hypochlorous acid building up in the bloodstream begins to bleach the iron out of heme and compete for O2 binding sites.
Red blood cells lose the ability to transport oxygen, causing the sufferer to turn blue in the face. Unliganded iron, hydrogen peroxide, and superoxide in the bloodstream undergo the Haber-Weiss and Fenton reactions, producing extremely reactive hydroxyl radicals that violently strip electrons from surrounding fats and DNA, oxidizing them severely.This condition is not unknown to medical science. The actual name for all of this is acute sepsis.We know this is happening in COVID-19 because people who have died of the disease have noticeable ferroptosis signatures in their tissues, as well as various other oxidative stress markers such as nitrotyrosine, 4-HNE, and malondialdehyde.When you intubate someone with this condition, you are setting off a free radical bomb by supplying the cells with O2.
It’s a catch-22, because we need oxygen to make Adenosine Triphosphate (that is, to live), but O2 is also the precursor of all these damaging radicals that lead to lipid peroxidation.The correct treatment for severe COVID-19 related sepsis is non-invasive ventilation, steroids, and antioxidant infusions. Most of the drugs repurposed for COVID-19 that show any benefit whatsoever in rescuing critically-ill COVID-19 patients are antioxidants. N-acetylcysteine, melatonin, fluvoxamine, budesonide, famotidine, cimetidine, and ranitidine are all antioxidants. Indomethacin prevents iron-driven oxidation of arachidonic acid to isoprostanes. There are powerful antioxidants such as apocynin that have not even been tested on COVID-19 patients yet which could defang neutrophils, prevent lipid peroxidation, restore endothelial health, and restore oxygenation to the tissues.
Scientists who know anything about pulmonary neutrophilia, ARDS, and redox biology have known or surmised much of this since March 2020. In April 2020, Swiss scientists confirmed that COVID-19 was a vascular endotheliitis. By late 2020, experts had already concluded that COVID-19 causes a form of viral sepsis. They also know that sepsis can be effectively treated with antioxidants. None of this information is particularly new, and yet, for the most part, it has not been acted upon. Doctors continue to use damaging intubation techniques with high PEEP settings despite high lung compliance and poor oxygenation, killing an untold number of critically ill patients with medical malpractice.Because of the way they are constructed, Randomized Control Trials will never show any benefit for any antiviral against COVID-19. Not Remdesivir, not Kaletra, not HCQ, and not Ivermectin. The reason for this is simple; for the patients that they have recruited for these studies, such as Oxford’s ludicrous RECOVERY study, the intervention is too late to have any positive effect.
The clinical course of COVID-19 is such that by the time most people seek medical attention for hypoxia, their viral load has already tapered off to almost nothing. If someone is about 10 days post-exposure and has already been symptomatic for five days, there is hardly any virus left in their bodies, only cellular damage and derangement that has initiated a hyperinflammatory response. It is from this group that the clinical trials for antivirals have recruited, pretty much exclusively.In these trials, they give antivirals to severely ill patients who have no virus in their bodies, only a delayed hyperinflammatory response, and then absurdly claim that antivirals have no utility in treating or preventing COVID-19. These clinical trials do not recruit people who are pre-symptomatic. They do not test pre-exposure or post-exposure prophylaxis. This is like using a defibrillator to shock only flatline, and then absurdly claiming that defibrillators have no medical utility whatsoever when the patients refuse to rise from the dead. The intervention is too late. These trials for antivirals show systematic, egregious selection bias. They are providing a treatment that is futile to the specific cohort they are enrolling.
COVID-19 is not a viral pneumonia. It is a viral vascular endotheliitis and attacks the lining of blood vessels, particularly the small pulmonary alveolar capillaries, leading to endothelial cell activation and sloughing, coagulopathy, sepsis, pulmonary edema, and ARDS-like symptoms. This is a disease of the blood and blood vessels. The circulatory system. Any pneumonia that it causes is secondary to that.In severe cases, this leads to sepsis, blood clots, and multiple organ failure, including hypoxic and inflammatory damage to various vital organs, such as the brain, heart, liver, pancreas, kidneys, and intestines.Some of the most common laboratory findings in COVID-19 are elevated D-dimer, elevated prothrombin time, elevated C-reactive protein, neutrophilia, lymphopenia, hypocalcemia, and hyperferritinemia, essentially matching a profile of coagulopathy and immune system hyperactivation/immune cell exhaustion.COVID-19 can present as almost anything, due to the wide tropism of SARS-CoV-2 for various tissues in the body’s vital organs.
While its most common initial presentation is respiratory illness and flu-like symptoms, it can present as brain inflammation, gastrointestinal disease, or even heart attack or pulmonary embolism.COVID-19 is more severe in those with specific comorbidities, such as obesity, diabetes, and hypertension. This is because these conditions involve endothelial dysfunction, which renders the circulatory system more susceptible to infection and injury by this particular virus. The vast majority of COVID-19 cases are mild and do not cause significant disease. In known cases, there is something known as the 80/20 rule, where 80% of cases are mild and 20% are severe or critical. However, this ratio is only correct for known cases, not all infections. The number of actual infections is much, much higher. Consequently, the mortality and morbidity rate is lower. However, COVID-19 spreads very quickly, meaning that there are a significant number of severely-ill and critically-ill patientsappearing in a short time frame.In those who have critical COVID-19-induced sepsis, hypoxia, coagulopathy, and ARDS, the most common treatments are intubation, injected corticosteroids, and blood thinners. This is not the correct treatment for COVID-19. In severe hypoxia, cellular metabolic shifts cause ATP to break down into hypoxanthine, which, upon the reintroduction of oxygen, causes xanthine oxidase to produce tons of highly damaging radicals that attack tissue. This is called ischemia-reperfusion injury, and it’s why the majority of people who go on a ventilator are dying. In the mitochondria, succinate buildup due to sepsis does the same exact thing; when oxygen is reintroduced, it makes superoxide radicals. Make no mistake,intubation will kill people who have COVID-19.
The end-stage of COVID-19 is severe lipid peroxidation, where fats in the body start to “rust” due to damage by oxidative stress. This drives autoimmunity. Oxidized lipids appear as foreign objects to the immune system, which recognizes and forms antibodies against OSEs, or oxidation-specific epitopes. Also, oxidized lipids feed directly into pattern recognition receptors, triggering even more inflammation and summoning even more cells of the innate immune system that release even more destructive enzymes.
This is similar to the pathophysiology of Lupus. COVID-19’s pathology is dominated by extreme oxidative stress and neutrophil respiratory burst, to the point where hemoglobin becomes incapable of carrying oxygen due to heme iron being stripped out of heme by hypochlorous acid. No amount of supplemental oxygen can oxygenate blood that chemically refuses to bind O2.The breakdown of the pathology is as follows:SARS-CoV-2 Spike binds to ACE2. Angiotensin Converting Enzyme 2 is an enzyme that is part of the renin-angiotensin-aldosterone system, or RAAS. The RAAS is a hormone control system that moderates fluid volume in the body and in the bloodstream (i.e. osmolarity) by controlling salt retention and excretion.
This protein, ACE2, is ubiquitous in every part of the body that interfaces with the circulatory system, particularly in vascular endothelial cells and pericytes, brain astrocytes, renal tubules and podocytes, pancreatic islet cells, bile duct and intestinal epithelial cells, and the seminiferous ducts of the testis, all of which SARS-CoV-2 can infect, not just the lungs.SARS-CoV-2 infects a cell as follows: SARS-CoV-2 Spike undergoes a conformational change where the S1 trimers flip up and extend, locking onto ACE2 bound to the surface of a cell. TMPRSS2, or transmembrane protease serine 2, comes along and cuts off the heads of the Spike, exposing the S2 stalk-shaped subunit inside. The remainder of the Spike undergoes a conformational change that causes it to unfold like an extension ladder, embedding itself in the cell membrane.
Then, it folds back upon itself, pulling the viral membrane and the cell membrane together. The two membranes fuse, with the virus’s proteins migrating out onto the surface of the cell. The SARS-CoV-2 nucleocapsid enters the cell, disgorging its genetic material and beginning the viral replication process, hijacking the cell’s own structures to produce more virus.SARS-CoV-2 Spike proteins embedded in a cell can actually cause human cells to fuse together, forming syncytia/MGCs (multinuclear giant cells). They also have other pathogenic, harmful effects. SARS-CoV-2’s viroporins, such as its Envelope protein, act as calcium ion channels, introducing calcium into infected cells. The virus suppresses the natural interferon response, resulting in delayed inflammation. SARS-CoV-2 N protein can also directly activate the NLRP3 inflammasome. Also, it suppresses the Nrf2 antioxidant pathway. The suppression of ACE2 by binding with Spike causes a buildup of bradykinin that would otherwise be broken down by ACE2.
This constant calcium influx into the cells results in (or is accompanied by) noticeable hypocalcemia, or low blood calcium, especially in people with Vitamin D deficiencies and pre-existing endothelial dysfunction. Bradykinin upregulates cAMP, cGMP, COX, and Phospholipase C activity. This results inprostaglandin release and vastly increased intracellular calcium signaling, which promotes highly aggressive ROS release and ATP depletion. NADPH oxidase releases superoxide into the extracellular space. Superoxide radicals react with nitric oxide to form peroxynitrite. Peroxynitrite reacts with the tetrahydrobiopterin cofactor needed by endothelial nitric oxide synthase, destroying it and “uncoupling” the enzymes, causing nitric oxide synthase to synthesize more superoxide instead.
This proceeds in a positive feedback loop until nitric oxide bioavailability in the circulatory system is depleted. Dissolved nitric oxide gas produced constantly by eNOS serves many important functions, but it is also antiviral against SARS-like coronaviruses, preventing the palmitoylation of the viral Spike protein and making it harder for it to bind to host receptors. The loss of NO allows the virus to begin replicating with impunity in the body. Those with endothelial dysfunction (i.e. hypertension, diabetes, obesity, old age, African-American race) have redox equilibrium issues to begin with, giving the virus an advantage.Due to the extreme cytokine release triggered by these processes, the body summons a great deal of neutrophils and monocyte-derived alveolar macrophages to the lungs.
Cells of the innate immune system are the first-line defenders against pathogens. They work by engulfing invaders and trying to attack them with enzymes that produce powerful oxidants, like SOD and MPO. Superoxide dismutase takes superoxide and makes hydrogen peroxide, and myeloperoxidase takes hydrogen peroxide and chlorine ions and makes hypochlorous acid, which is many, many times more reactive than sodium hypochlorite bleach.Neutrophils have a nasty trick. They can also eject these enzymes into the extracellular space, where they will continuously spit out peroxide and bleach into the bloodstream. This is called neutrophil extracellular trap formation, or, when it becomes pathogenic and counterproductive, NETosis. In severe and critical COVID-19, there is actually rather severe NETosis.Hypochlorous acid building up in the bloodstream begins to bleach the iron out of heme and compete for O2 binding sites.
Red blood cells lose the ability to transport oxygen, causing the sufferer to turn blue in the face. Unliganded iron, hydrogen peroxide, and superoxide in the bloodstream undergo the Haber-Weiss and Fenton reactions, producing extremely reactive hydroxyl radicals that violently strip electrons from surrounding fats and DNA, oxidizing them severely.This condition is not unknown to medical science. The actual name for all of this is acute sepsis.We know this is happening in COVID-19 because people who have died of the disease have noticeable ferroptosis signatures in their tissues, as well as various other oxidative stress markers such as nitrotyrosine, 4-HNE, and malondialdehyde.When you intubate someone with this condition, you are setting off a free radical bomb by supplying the cells with O2.
It’s a catch-22, because we need oxygen to make Adenosine Triphosphate (that is, to live), but O2 is also the precursor of all these damaging radicals that lead to lipid peroxidation.The correct treatment for severe COVID-19 related sepsis is non-invasive ventilation, steroids, and antioxidant infusions. Most of the drugs repurposed for COVID-19 that show any benefit whatsoever in rescuing critically-ill COVID-19 patients are antioxidants. N-acetylcysteine, melatonin, fluvoxamine, budesonide, famotidine, cimetidine, and ranitidine are all antioxidants. Indomethacin prevents iron-driven oxidation of arachidonic acid to isoprostanes. There are powerful antioxidants such as apocynin that have not even been tested on COVID-19 patients yet which could defang neutrophils, prevent lipid peroxidation, restore endothelial health, and restore oxygenation to the tissues.
Scientists who know anything about pulmonary neutrophilia, ARDS, and redox biology have known or surmised much of this since March 2020. In April 2020, Swiss scientists confirmed that COVID-19 was a vascular endotheliitis. By late 2020, experts had already concluded that COVID-19 causes a form of viral sepsis. They also know that sepsis can be effectively treated with antioxidants. None of this information is particularly new, and yet, for the most part, it has not been acted upon. Doctors continue to use damaging intubation techniques with high PEEP settings despite high lung compliance and poor oxygenation, killing an untold number of critically ill patients with medical malpractice.Because of the way they are constructed, Randomized Control Trials will never show any benefit for any antiviral against COVID-19. Not Remdesivir, not Kaletra, not HCQ, and not Ivermectin. The reason for this is simple; for the patients that they have recruited for these studies, such as Oxford’s ludicrous RECOVERY study, the intervention is too late to have any positive effect.
The clinical course of COVID-19 is such that by the time most people seek medical attention for hypoxia, their viral load has already tapered off to almost nothing. If someone is about 10 days post-exposure and has already been symptomatic for five days, there is hardly any virus left in their bodies, only cellular damage and derangement that has initiated a hyperinflammatory response. It is from this group that the clinical trials for antivirals have recruited, pretty much exclusively.In these trials, they give antivirals to severely ill patients who have no virus in their bodies, only a delayed hyperinflammatory response, and then absurdly claim that antivirals have no utility in treating or preventing COVID-19. These clinical trials do not recruit people who are pre-symptomatic. They do not test pre-exposure or post-exposure prophylaxis. This is like using a defibrillator to shock only flatline, and then absurdly claiming that defibrillators have no medical utility whatsoever when the patients refuse to rise from the dead. The intervention is too late. These trials for antivirals show systematic, egregious selection bias. They are providing a treatment that is futile to the specific cohort they are enrolling.
Guest- Guest
Re: Korona novosti i spoznaje
by ljubo1212 24/10/2021, 19:04
i danas je među umrlima preko 60% jabuka
u oboljelom voću danas jabuke čine oko 75%
sve pohvale necijepljenom voću, voćkama i voćarima
u oboljelom voću danas jabuke čine oko 75%
sve pohvale necijepljenom voću, voćkama i voćarima

ljubo1212- Posts : 2050
2015-08-02
Re: Korona novosti i spoznaje
by Guest 24/10/2021, 19:15
ljubo1212 wrote:i danas je među umrlima preko 60% jabuka
u oboljelom voću danas jabuke čine oko 75%
sve pohvale necijepljenom voću, voćkama i voćarima
Ti se pojavis samo da istovaris svoju balegu.
Guest- Guest
Re: Korona novosti i spoznaje
by ljubo1212 24/10/2021, 19:20
što čekaju oni tvoji profesori? nikako objaviti najavljenu ekskluzivnu studiju? hebga, prošlo skoro pola godine, zakasnit će za nobela
ljubo1212- Posts : 2050
2015-08-02
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 19:23
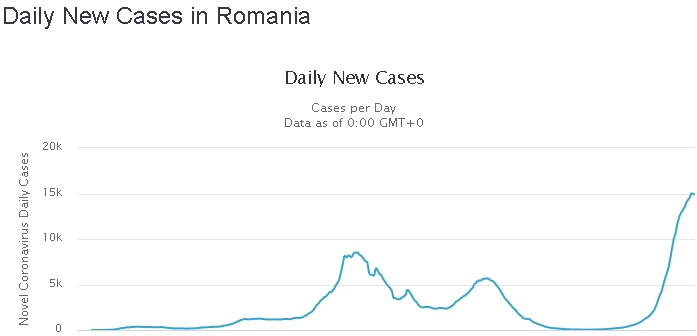
Mislim da smo ovdje Rumuniju spominjali već prije kakvih par tjedana.
Već tada smo rekli da će im biti potrebna pomoć.
Zdravstveno osoblje im radi po 100h na tjedan, nema respiratora itd
Efektivna procjepljenost ima je cca 21%.
Situacija im je pobjegla iz kontrole, u covid bolnicama vele da s mrtvima nemaju kud...
Obratite pažnu na naklon krivule rasta zaraze, kao i rasta umrlih.

Već tada smo rekli da će im biti potrebna pomoć.
Zdravstveno osoblje im radi po 100h na tjedan, nema respiratora itd
Efektivna procjepljenost ima je cca 21%.
Situacija im je pobjegla iz kontrole, u covid bolnicama vele da s mrtvima nemaju kud...
Obratite pažnu na naklon krivule rasta zaraze, kao i rasta umrlih.
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Guest 24/10/2021, 19:25
ljubo1212 wrote:što čekaju oni tvoji profesori? nikako objaviti najavljenu ekskluzivnu studiju? hebga, prošlo skoro pola godine, zakasnit će za nobela
Majmune rvacki vec sam stavio nastavak ali ti ne pratis nego se klanjas sliji Ante Pavelica.
Trazi sam gdje su dokumenti koje sam nedavno stavio ovdje.
Guest- Guest
Re: Korona novosti i spoznaje
by ljubo1212 24/10/2021, 19:29
ajd nađi, dobiješ sljedovanje sijena...
pavelić? i onda napadate čoporativno eru, hebalo nanu
pavelić? i onda napadate čoporativno eru, hebalo nanu
ljubo1212- Posts : 2050
2015-08-02
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 19:29
Slična situacioja je i u Bugarskoj.
Efektivna procijepljenost 18.4%
Traže pomoć, kao i Rumunji!


Efektivna procijepljenost 18.4%
Traže pomoć, kao i Rumunji!
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Guest 24/10/2021, 19:31
ljubo1212 wrote:ajd nađi, dobiješ sljedovanje sijena...
pavelić? i onda napadate čoporativno eru, hebalo nanu
Nađi sam. Nemam vremena se zajebavati sa rvackim nepismenim psihopatama.
Guest- Guest
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 19:33
PS.:
Poslije ćemo pogledati kako izgledaju HR dijagrami.
Poslije ćemo pogledati kako izgledaju HR dijagrami.
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Guest 24/10/2021, 19:40
Eroo wrote:PS.:
Poslijećemopogledati kako izgledaju HR dijagrami.
ćeš
Jer te tvoje škrabotine od dijagrama nitko ne gleda.
Guest- Guest
T.- Posts : 17557
2014-04-14
Age : 83
Re: Korona novosti i spoznaje
by mutava baštarda 24/10/2021, 19:58
prckov wrote:danas je 60% preminulih od COVID-a u posljednja 24 sata bilo necijepljeno.
ok, to znaci da je 40% necjepljenih prezivilo
Koliki postotak umrlih je bio cijepljen?
njih nije niko ni pomeno
greska, 60% preminulih od covida, ja sam mislio necjepljenih
u tom slucaju treba se znat tocan broj jednih i drugih

40% smrti od kovida otpada na 43% cijepljene populacije.
Ide to pomalo. Još malo pa će biti ka Engleska i Škotska.
_________________
Iduća dva tjedna su ključna
mutava baštarda- Posts : 21037
2015-09-14
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 19:59
Živio, rođo, dugo te nije bilo na ovom forum-balonu.ljubo1212 wrote:ajd nađi, dobiješ sljedovanje sijena...
pavelić? i onda napadate čoporativno eru, hebalo nanu
U zdnje vrijeme smo postali fini pa sad čopor sad nazivamo balonom.
Inače ovi iz balona sad preživlju nakon šta su dobili svoj naramak.
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 20:06
mutava baštarda wrote:prckov wrote:danas je 60% preminulih od COVID-a u posljednja 24 sata bilo necijepljeno.
ok, to znaci da je 40% necjepljenih prezivilo
Koliki postotak umrlih je bio cijepljen?
njih nije niko ni pomeno
greska, 60% preminulih od covida, ja sam mislio necjepljenih
u tom slucaju treba se znat tocan broj jednih i drugih
40% smrti od kovida otpada na 43% cijepljene populacije.
Ide to pomalo. Još malo pa će biti ka Engleska i Škotska.
Smušeno kao i obično. Niđe veze...
Uostalom, uputi nas na link gdje su objavljeni podatci koje navodite.
Nemate ga? Tako sam i mislio...
Sad možeš izvoditi razne zaključke, meni svejedno...
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 20:07
Sad kad krene c.p. memova, smiješnica i videa s izjavama raznih "uglednih" znanstvenika... 
_________________
Nulla rosa sine spina
Eroo- Posts : 78946
2016-07-22
Re: Korona novosti i spoznaje
by Eroo 24/10/2021, 20:11
Eroo wrote:Mislim da smo ovdje Rumuniju spominjali već prije kakvih par tjedana.
Već tada smo rekli da će im biti potrebna pomoć.
Zdravstveno osoblje im radi po 100h na tjedan, nema respiratora itd
Efektivna procjepljenost ima je cca 21%.
Situacija im je pobjegla iz kontrole, u covid bolnicama vele da s mrtvima nemaju kud...
Obratite pažnu na naklon krivule rasta zaraze, kao i rasta umrlih.
21% cijepljenih s 2doze.
Rezultat je tu.
Eroo- Posts : 78946
2016-07-22
Page 27 of 50 • 1 ... 15 ... 26, 27, 28 ... 38 ... 50 ![]()
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
» Korona novosti i spoznaje
Page 27 of 50
Permissions in this forum:
You cannot reply to topics in this forum